

Supplemental Digital Content is available in the text.
Abstract
Background:
There is an unknown percentage of transgender and gender non-confirming individuals who undergo gender-affirmation surgeries (GAS) that experiences regret. Regret could lead to physical and mental morbidity and questions the appropriateness of these procedures in selected patients. The aim of this study was to evaluate the prevalence of regret in transgender individuals who underwent GAS and evaluate associated factors.
Methods:
A systematic review of several databases was conducted. Random-effects meta-analysis, meta-regression, and subgroup and sensitivity analyses were performed.
Results:
A total of 27 studies, pooling 7928 transgender patients who underwent any type of GAS, were included. The pooled prevalence of regret after GAS was 1% (95% CI <1%–2%). Overall, 33% underwent transmasculine procedures and 67% transfemenine procedures. The prevalence of regret among patients undergoing transmasculine and transfemenine surgeries was <1% (IC <1%–<1%) and 1% (CI <1%–2%), respectively. A total of 77 patients regretted having had GAS. Twenty-eight had minor and 34 had major regret based on Pfäfflin’s regret classification. The majority had clear regret based on Kuiper and Cohen-Kettenis classification.
Conclusions:
Based on this review, there is an extremely low prevalence of regret in transgender patients after GAS. We believe this study corroborates the improvements made in regard to selection criteria for GAS. However, there is high subjectivity in the assessment of regret and lack of standardized questionnaires, which highlight the importance of developing validated questionnaires in this population.
Introduction
Discordance or misalignment between gender identity and sex assigned at birth can translate into disproportionate discomfort, configuring the definition of gender dysphoria.1–3 This population has increased risk of psychiatric conditions, including depression, substance abuse disorders, self-injury, and suicide, compared with cis-gender individuals.4,5 Approximately 0.6% of adults in the United States identify themselves as transgenders.6 Despite advocacy to promote and increase awareness of the human rights of transgender and gender non-binary (TGNB) individuals, discrimination continue to afflict the daily life of these individuals.4,7
Gender-affirmation care plays an important role in tackling gender dysphoria.5,8–10 Gender-affirmation surgeries (GAS) aim to align the patients’ appearance with their gender identity and help achieve personal comfort with one-self, which will help decrease psychological distress.5,10 These interventions should be addressed by a multidisciplinary team, including psychiatrists, psychologists, endocrinologists, physical therapists, and surgeons.1,9 The number of GAS has consistently increased during the last years. In the United States, from 2017 to 2018, the number of GAS increased to 15.3%.8,11,12
Significant improvement in the quality of life, body image/satisfaction, and overall psychiatric functioning in patients who underwent GAS has been well documented.5,13–19 However, despite this, there is a minor population that experiences regret, occasionally leading to de-transition surgeries.20 Both regret and de-transition may add an important burden of physical, social, and mental distress, which raises concerns about the appropriateness and effectiveness of these procedures in selected patients. Special attention should be paid in identifying and recognizing the prevalence and factors associated with regret. In the present study, we hypothesized that the prevalence of regret is less than the last estimation by Pfafflin in 1993, due to improvements in standard of care, patient selection, surgical techniques, and gender confirmation care. Therefore, the aim of this study was to evaluate the prevalence of regret and assess associated factors in TGNB patients 13-years-old or older who underwent GAS.20
Methods
Search Methodology
Following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines, a comprehensive research of several databases from each database’s inception to May 11, 2020, for studies in both English and Spanish languages, was conducted.21 The databases included Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, and Daily, Ovid EMBASE, Ovid Cochrane Central Register of Controlled Trials, Ovid Cochrane Database of Systematic Reviews, and Scopus. The search strategy was designed and conducted by an experienced librarian, with input from the study’s principal investigator. Controlled vocabulary supplemented with keywords was used to search for studies of de-transition and regret in adult patients who underwent gender confirmation surgery. The actual strategy listing all search terms used and how they are combined is available in Supplemental Digital Content 1. (See Supplemental Digital Content 1, which displays the search strategy. http://links.lww.com/PRSGO/B598.)
Study Selection
Search results were exported from the database into XML format and then uploaded to Covidence.22 The study selection was performed in a 2-stage screening process. The first step was conducted by 2 screeners (V.P.B. and S.S.B.), who reviewed titles and abstracts and selected those of relevance to the research question. Then, the same 2 screeners reviewed full text of the remaining articles and selected those eligible according to the inclusion and exclusion criteria (Fig. 1). If disagreements were encountered, a third reviewer (O.J.M.) moderated a discussion, and a joint decision between the 3 reviewers was made for a final determination. Inclusion criteria were all the articles that included patients aged 13 years or more who underwent GAS and report regret or de-transition rates, and observational or interventional studies in English or Spanish language. Exclusion criteria were letter to the editors, case series with <10 patients, case reports correspondences, and animal studies.
Fig. 1.
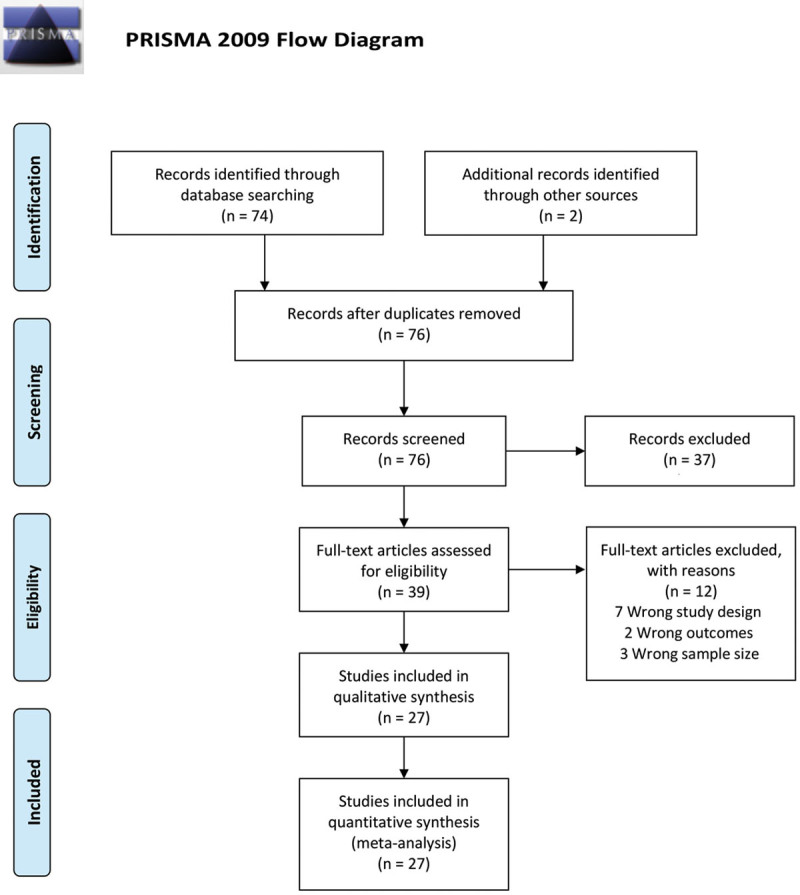
PRISMA flow diagram for systematic reviews.
Data Extraction/Synthesis
After selecting the articles, we assessed study characteristics. We identified year of publication, country in which the study was conducted, population size, and number of transmasculine and transfemenine patients with their respective mean age (expressed with SD, range, or interquartile range if included in the study). In addition, we extracted information of the method of data collection (interviews versus questionnaires), number of regrets following GAS, as well as the type of surgery, time of follow-up, and de-transition procedures. We classified the type of regret based on the patient’s reasons for regret if they were mentioned in the studies. We used the Pfäfflin and Kuiper and Cohen-Kettenis classifications of regret (Table 1).20,23
Table 1.
Pfäfflin and Kuiper and Cohen-Kettenis Categories of Regret
| Pfäfflin, 1993 | Minor | Feeling of regret secondary to surgical complications or social problems. |
| Major | “True” regret. Feeling of dysphoria secondary to the new appearance, or desires of pursuing a de-transition surgery. | |
| Kuiper and Cohen-Kettenis, 1998 | Clear regret | Patients openly express their regret and have role reversal either by undergoing de-transition surgery or returning to their former gender role. |
| Regret uncertain | Patients don’t have role reversal, but freely express their regret by never considering doing GAS or pass through the same preoperative scenario again. They are truly disappointed with the results of GAS. Also, they don’t consider the new gender role so difficult and might consider a second GAS. | |
| Regret | Patients have role reversal but don’t express their feelings of regret. Some might state that they are happy about their decision and consider themselves as transgender. However, they live as their former gender role for practical and social reasons. | |
| Regret assumed by others | Don’t have role reversal and don’t express feelings of regret but have unfavorable social circumstances or psychological disturbances that raise concerns to relatives, clinicians, and others that patient might be regretful (eg, feeling loneliness, suicide attempts). |
Quality Assessment
To assess the risk of bias within each study, the National Institute of Health (NIH) quality assessment tool was used.24 This tool ranks each article as “good,” “fair,” or “poor,” and with this, we categorized each article into “low risk,” “moderate risk,” or “high risk” of bias, respectively.
Outcomes
Our primary outcome of interest was the prevalence of regret of transgender patients who underwent any type of GAS. Secondary outcomes of interest were discriminating the prevalence of regrets by type gender transition (transfemenine and transmasculine), and type of surgery.
Data Analysis and Synthesis
The binominal data were analyzed, and the pooled prevalence of regret was estimated using proportion meta-analysis with Stata Software/IC (version 16.1).25 Given the heterogeneity between studies, we conducted a logistic-normal-random-effect model. The study-specific proportions with 95% exact CIs and overall pooled estimates with 95% Wald CIs with Freeman-Turkey double arcsine transformation were used. The effect size and percentage of weight were presented for each individual study.25,26
To evaluate heterogeneity, I2 statistics was used. If P < 0.05 or I2 > 50%, significant heterogeneity was considered. A univariate meta-regression analysis was performed to assess the significance in country of origin, tools of measurement, and quality of the studies.
To assess publication bias, we used funnel plot graphic and the Egger test. If this test showed us no statistical significance (P > 0.05), we assumed that the publication bias had a low impact on the results of our metanalysis. To assess the impact of the publication bias on our missing studies, we used the trim-and-fill method.
A sensitivity analysis was conducted to assess the influence of certain characteristics in the magnitude and precision of the overall prevalence of regret. The following characteristics were excluded: <10 participants included, and the presence of a high risk of bias.
Results
Study Selection
A total of 74 articles were identified in the search, and 2 additional records were identified through other sources. After the first-step screening process, 39 articles were relevant based on the information provided in their titles and abstracts. After the second-step process, a total of 27 articles were included in the systematic review and metanalysis (Fig. 1).
Quality Assessment
Based on the NIH quality assessment tool, the majority of article ranged between “poor” and “fair” categories.24 (See Supplemental Digital Content 2, which displays the score of each reviewed study. http://links.lww.com/PRSGO/B599.)
Study Characteristics
In total, the included studies pooled 7928 cases of transgender individuals who underwent any type of GAS. A total of 2578 (33%) underwent transmasculine procedures, 5136 (67%) underwent transfemenine surgeries, and 1 non-binary patient underwent surgery. In Table 2 characteristics of studies are listed. Without discriminating type of surgical technique, from all transfemenine surgeries included, 772 (39.3%) were vaginoplasty, 260 (13.3%) were clitoroplasty, 107 (5.5%) were breast augmentation, 72 (3.7%) were labioplasty and vulvoplasty, and a small minority were facial feminization surgery, vocal cord surgery, thyroid cartilage reduction, and oophorectomy surgery. The rest did not specify type of surgery. In regard to transmasculine surgeries, 297 (12.4%) were mastectomies, 61 (2.6%) were phalloplasties, and 51 (2.1%) hysterectomies (Table 3 and 4). Overall, follow-up time from surgery to the time of regret assessment ranged from 0.8 to 9 years (Table 2).
Table 2.
Study Characteristics
| Authors and Year of Publication | Country | Sample Size | Transmasculine | Mean Age (y) | Transfemenine | Mean Age (y) | Mean Follow-up (y) | Assessment Tool | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|
| Blanchard et al, 1989 | Canada | 111 | 61 | 28.5 | 50 | 41.4 (He), 29.0 (Ho) | 4.4 | Q | H |
| Bouman, 1988 | Netherlands | 55 | NA | NA | 55 | NS | 2.3 | NS | M |
| Cohen-Kettenis et al, 1997 | Netherlands | 19 | 14 | 22* | 5 | 22* | 2.6 | I | H |
| De Cuypere et al, 2006 | Belgium | 62 | 27 | 33.3 | 35 | 41.4 | Transmasculine = 7.6 | I | M |
| Transfemenine = 4.1 | |||||||||
| Garcia et al, 2014 | London | 25 | 25 | 34 –RAP without | NA | NA | RAP without = 6.8 | I | H |
| 39.2 – RAP | RAP = 2.2 | ||||||||
| 35.1 – SP | SP = 2.2 | ||||||||
| Imbimbo et al, 2009 | Italia | 139 | NA | NA | 139 | 31.4 | 1–1.6 | Q | H |
| Jiang et al, 2018 | USA | 80 | NA | NA | 79 (+ 1 NB) | 57.9 – Vulvoplasty | 0.7 | NS | H |
| 39.2 – Vaginoplasty† | |||||||||
| Johansson et al, 2010 | Sweden | 32 | 14 | 38.9 | 18 | 46 | 9 | Q/I | L |
| Krege et al, 2001 | Germany | 31 | NA | NA | 31 | Me 36.9 | 0.5 | Q | H |
| Kuiper et al, 1998 | Netherlands | 1100 | 300 | 46.4* | 800 | 46.4* | NS | Q | H |
| Lawrence, 2003 | USA | 232 | NA | NA | 232 | 44 | 3 | Q | M |
| Lobato et al, 2006 | Brazil | 19 | 1 | 31.2* | 18 | 31.2* | 2.1 | Q/I | M |
| Nelson et al, 2009 | UK | 17 | 17 | 31 | NA | NA | 0.8 | Q | M |
| Olson-Kennedy et al, 2018 | USA | 68 | 68 | 18.9 | NA | NA | <1–5 | Q | M |
| Papadopulos et al, 2017 | Germany | 47 | NA | NA | 47 | 38.3 | 1.6 | Q | L |
| Pfafflin, 1993 | Germany | 295 | 99 | NS | 196 | NS | Range: 1–29 | NS | M |
| Rehman et al, 1999 | USA | 28 | NA | NA | 28 | 38.0 | NS | Q | L |
| Smith et al, 2001 | Netherlands | 20 | 13 | 21* | 7 | 21* | 1.3 | I | M |
| Song et al, 2011 | Singapore | 19 | 19 | NS | NA | NA | Range: 1–10 | Q | H |
| Van de Grift et al, 2018 | Netherlands, Belgium, Germany, Norway | 132 | 51 | 36.3* | 81 | 36.3* | NS | Q | M |
| Wiepjes et al, 2018 | Netherlands | 4863 | 1733 | Adults: Me 23 | 3130 | Adults: Me 33 | 8.5 | Q | M |
| Adolescents: Me 26 | Adolescents: Me 16 | ||||||||
| Zavlin et al, 2018 | Germany | 40 | NA | NA | 40 | 38.6 | 0.9 | Q | M |
| Judge et al, 2014 | Ireland | 55 | 19 | 32.2‡ | 36 | 36.2‡ | NS | I | M |
| Vujovic et al, 2009 | Serbia | 118 | 59 | 25.7 | 59 | 25.4 | NS | NS | H |
| Weyers et al, 2009 | Belgium | 50 | NA | NA | 50 | 43.1 | 6.3 | Q | L |
| Poudrier et al, 2019 | USA | 58 | 58 | 33 | NA | NA | NS | Q | M |
| Laden et al, 1998 | Sweden | 213 | NS | NS | NS | NS | NS | Medical records and verdicts | M |
*Reflects the mean of both transmasculine and transfemenine.
†Includes both scheduled and completed surgery.
‡Includes both surgery and no surgery patients.
H, High; He, Heterosexual; Ho, Homosexual; I, Interview; IQR, Interquartile Range; L, Low; M, Moderate; Me, Median; NA, Not applicable; NS: Not specified, Q: Questionnaire; RAP: Radial Arterial Forearm-Flap Phalloplasty without or with cutaneous nerve to clitoral nerve anastomosis; SP: Suprapubic Pedicle-Flap Phalloplasty.
Table 3.
Studies Differentiating Type of Surgery among Transfemenine Patients
| Type of Surgery | No. Procedures |
|---|---|
| Breast Augmentation | |
| Smith et al, 2001 | 7 |
| Van de Grift et al, 2018 | 33 |
| Judge et al, 2014 | 19 |
| Weyers et al, 2009 | 48 |
| Total | 107 |
| Vaginoplasty | |
| Blanchard et al, 1989 | 50 |
| Bouman, 1988 | 7 |
| Cohen-Kettenis et al, 1997 | 5 |
| Imbimbo et al, 2009 | 139 |
| Jiang et al, 2018 | 64 |
| Krege et al, 2001 | 31 |
| Kuiper et al, 1998 | 8 |
| Lawrence, 2003 | 232 |
| Papadopulos et al, 2017 | 47 |
| Rehman et al, 1999 | 28 |
| Van de Grift et al, 2018 | 71 |
| Zavlin et al, 2018 | 40 |
| Weyers et al, 2009 | 50 |
| Total | 772 |
| Vulvoplasty | |
| Rehman et al, 1999 | 28 |
| Jiang et al, 2018 | 16 |
| Total | 44 |
| Others | |
| Lawrence, 2003 | Clitoroplasty 232 |
| Rehman et al, 1999 | Clitoroplasty + labioplasty 28 + Orchiectomy 5 |
| Van de Grift et al, 2018 | Thyroid cartilage reduction 9, facial surgeries 7, and vocal cord 3 |
| Wiepjes et al, 2018 | Gonadectomy 2868 (adults), 262 (adolescents) |
| Judge et al, 2014 | Facial surgeries 6, laryngeal surgeries 2, GAS not specified 15 |
| Weyers et al, 2009 | Vocal cord surgeries 20, cricoid reduction 15 |
Table 4.
Studies Differentiating the Type of Surgery among Transmasculine Patients
| Type of Surgery | No. Procedures |
|---|---|
| Mastectomy | |
| Blanchard et al, 1989 | 61 |
| Cohen-Kettenis et al, 1997 | 14 |
| Kuiper et al, 1998 | 1 |
| Nelson et al, 2009 | 17 |
| Olson-Kennedy et al, 2018 | 68 |
| Smith et al, 2001 | 13 |
| Van de Grift et al, 2018 | 49 |
| Judge et al, 2014 | 16 |
| Poudrier et al, 2019 | 58 |
| Total | 297 |
| Phalloplasty | |
| Cohen-Kettenis et al, 1997 | 1 |
| Garcia et al, 2014 | 25 |
| Smith et al, 2001 | 1 |
| Song et al, 2011 | 19 |
| Van de Grift et al, 2018 | 15 |
| Total | 61 |
| Hysterectomy | |
| Kuiper et al, 1998 | 1 |
| Smith et al, 2001 | 2 |
| Van de Grift et al, 2018 | 48 |
| Total | 51 |
| Others | |
| Cohen-Kettenis et al, 1997 | Neoscrotum 2 |
| Kuiper et al, 1998 | Oophorectomy 1 |
| Van de Grift et al, 2018 | Metoidioplasty 3 |
| Wiepjes et al, 2018 | Gonadectomy 1361 (adults), 372 (adolescents) |
| Judge et al, 2014 | GAS not specified 9 |
Regrets and De-transition
Almost all studies conducted non-validated questionnaires to assess regret due to the lack of standardized questionnaires available in this topic.15, 19–33 Most of the questions evaluating regret used options such as, “yes,” “sometimes,” “no” or “all the time,” “sometimes,” “never,” or “most certainly,” “very likely,” “maybe,” “rather not,” or “definitely not.”14, 18, 19, 23, 27–38 Other studies used semi-structured interviews.34,37,39–43 However, in both circumstances, some studies provided further specific information on reasons for regret.14,20,23,29,32,36,41,44–46 Of the 7928 patients, 77 expressed regret (12 transmen, 57 transwomen, 8 not specified), understood by those who had “sometimes” or “always” felt it.
Reasons for Regret
The most prevalent reason for regret was the difficulty/dissatisfaction/acceptance in life with the new gender role.23,29,32,36,44 Other less prevalent reasons were “failure” of surgery to achieve their surgical goals in an aesthetic level and psychological level.29,32,36,47 Based on the reasons presented, we classified the types of regrets according to Pfäfflin’s types of regret and Kuiper and Cohen-Kettenis classification. According to Pfäfflin’s types, 28 patients had minor regret, and 34 patients had major regret.14,20,23,29,32,36,41,44,45 Based on the Kuiper and Cohen-Kettenis regret classification, 35 patients had clear regret, 26 uncertain regret, 1 regret, and none presented with regret assumed by others.23 In Table 5 and 6, the reasons and classifications are shown.
Table 5.
Type of Regret
| Studies | No. Regrets | Transmasculine | Transfeminine | Type of Regrets based on Pfafflin, 1993 | Type of Regrets based on Kuiper and Cohen-Kettenis, 1998 | Surgery | De-transition (Y/N) | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Minor | Major | 1 | 2 | 3 | 4 | ||||||
| Blanchard et al, 1989 | 4 | — | 4 | 4 | — | 2 | 2 | — | — | Vaginoplasty | N |
| Bouman, 1988 | 1 | — | 1 | — | 1 | 1 | — | — | — | Vaginoplasty | NS |
| De Cuypere et al, 2006 | 2 | 1 | 1 | 2 | — | — | 2 | — | — | NS | NS |
| Imbimbo et al, 2009 | 8 | — | 8 | NS | NS | NS | NS | NS | NS | Vaginoplasty | NS |
| Jiang et al, 2018 | 1 | — | 1 | 1 | — | — | 1 | — | — | Vulvoplasty | NS |
| Kuiper et al, 1998 | 10 | 1 | 9 | 4 | 6 | 6 | 3 | 1 | — | NS | 1 testicles implant removal and underwent breast augmentation |
| Lawrence, 2003 | 15 | — | 15 | 13 | 2 | 2 | 13 | — | — | Vaginoplasty | NS |
| Olson-Kennedy et al, 2018 | 1 | 1 | — | NS | NS | NS | NS | NS | NS | Mastectomy | NS |
| Pfafflin, 1993 | 3 | 3 | — | — | 3 | 3 | — | — | — | NS (complication urethral-vaginal fistula) | NS |
| Van de Grift et al, 2018 | 2 | 1 | 1 | 2 | — | — | 2 | — | — | Transfemenine = Vaginoplasty Transmasculine = mastectomy and uterus extirpation (hematoma) | NS |
| Wiepjes et al, 2018 | 14 | 3 | 11 | 0 | 14 | 13 | 1 | 0 | 0 | Gonadectomy | Y (10)* |
| Zavlin et al, 2018 | 1 | — | 1 | NS | NS | NS | NS | NS | NS | Vaginoplasty | NS |
| Judge et al, 2014 | 3 | — | 3 | NS | NS | NS | NS | NS | NS | NS | NS |
| Weyers et al, 2009 | 2 | — | 2 | NS | NS | NS | NS | NS | NS | Vaginoplasty | NS |
| Poudrier et al, 2019 | 2 | 2 | — | 2 | — | — | 2 | — | — | Mastectomy | NS |
| Laden et al, 1998 | 8 | NS | NS | — | 8 | 8 | — | — | — | NS | Y |
*8 mastectomies, 2 vaginectomies, 2 phalloplasties, 2 testicular implants removal, and 1 breast augmentation.
N, no; NS, not specified; Y, Yes.
Table 6.
Causes of Regret
| Studies | Reasons of Regrets |
|---|---|
| Blanchard et al, 1989 | • 1 patient was dissatisfied with life as a woman and considered returning to the masculine role |
| • 1 patient reported that surgery failed to produce the coherence of mind and the body he wanted | |
| • 1 patient would not opt for a new surgery as it had not accomplished what she wanted | |
| • 1 patient dressed as a man but didn’t felt as feminine nor masculine | |
| Bouman, 1988 | Work and social acceptance |
| De Cuypere et al, 2006 | • Transmasculine = Physiologic period before GAS (delusional disorder-erotomaniac type), scored very low in credibility |
| • Transfemenine = Emotionally troubled by a break-up with his girlfriend | |
| Imbimbo et al, 2009 | NS |
| Jiang et al, 2018 | Didn’t want to wait genital electrolysis prior vaginoplasty |
| Kuiper et al, 1998 | • 4 patients mentioned they were not transsexual |
| • 1 patient after surgery she realized she did not want to live as a woman. 1 never wished for the surgery (forced by the partner) | |
| • 2 patients lost the partner and had social problems | |
| • 1 patient had no doubts (double role requested by the partner) | |
| Lawrence, 2003 | • 8 patients felt disappointed with physical or functional outcomes of surgery (lost clitoris sensation) |
| • 2 participants reported reversion to living as a man after GAS. There were family and social problems | |
| Olson-Kennedy et al, 2018 | NS |
| Pfafflin, 1993 | NS |
| Van de Grift et al, 2018 | • Transmasculine = Body does not meet the feminine ideal |
| • Transfemenine = Recurrent abdominal pains, dependence on exogenous hormones | |
| Wiepjes et al, 2018 | • 5 patients had social regret (still as their former role/“ignored by surroundings” or “the loss of relatives is a large sacrifice”) |
| • 7 patients had true regret (though that the surgery was the solution) | |
| • 2 patients felt non-binary | |
| Zavlin et al, 2018 | NS |
| Judge et al, 2014 | NS |
| Weyers et al, 2009 | NS |
| Poudrier et al, 2019 | Aesthetic outcomes |
| Laden et al, 1998 | NS |
NS, not specified.
Prevalence of Regret
The pooled prevalence of regret among the TGNB population after GAS was 1% (95% Confidence interval [CI] <1%–2%; I2 = 75.1%) (Fig. 2). The prevalence for transmasculine surgeries was <1% (CI <1%–<1%, I2 = 28.8%), and for transfemenine surgeries, it was 1% (CI <1%–2%, I2 = 75.5%) (Fig. 3). The prevalence of regret after vaginoplasty was of 2% (CI <1%–4%, I2 = 41.5%) and that after mastectomy was <1% (CI <1–<1%, I2 = 21.8%) (Fig. 4).
Fig. 2.
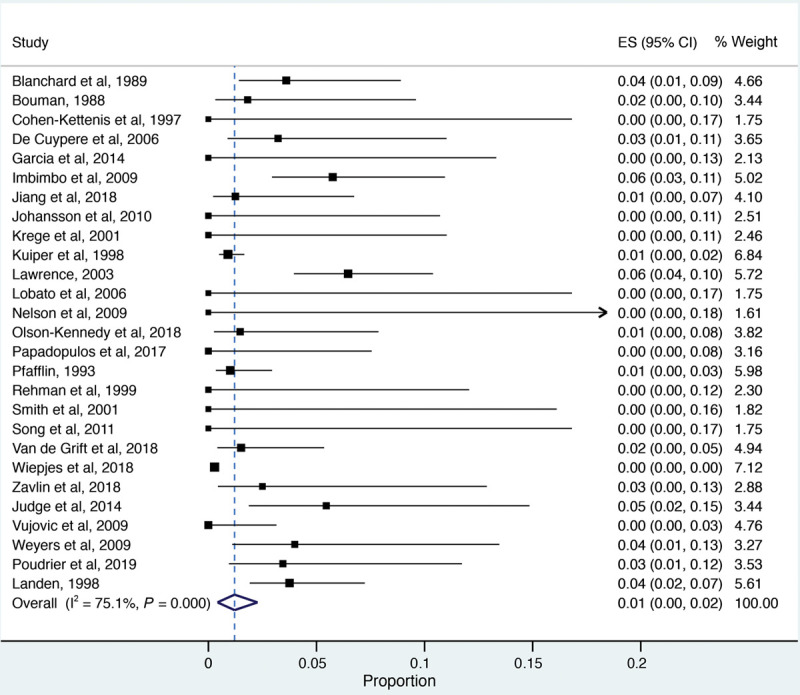
Pooled prevalence of regret among TGNB individuals after gender confirmation surgery. Heterogeneity χ2 = 104.31 (d.f. = 26), P = 0.00, I2 [variation in effect size (ES) attributable to heterogeneity] = 75.08%, Estimate of between-study variance Ʈ2 = 0.02, Test of ES = 0, z = 4.22, P = 0.00.
Fig. 3.
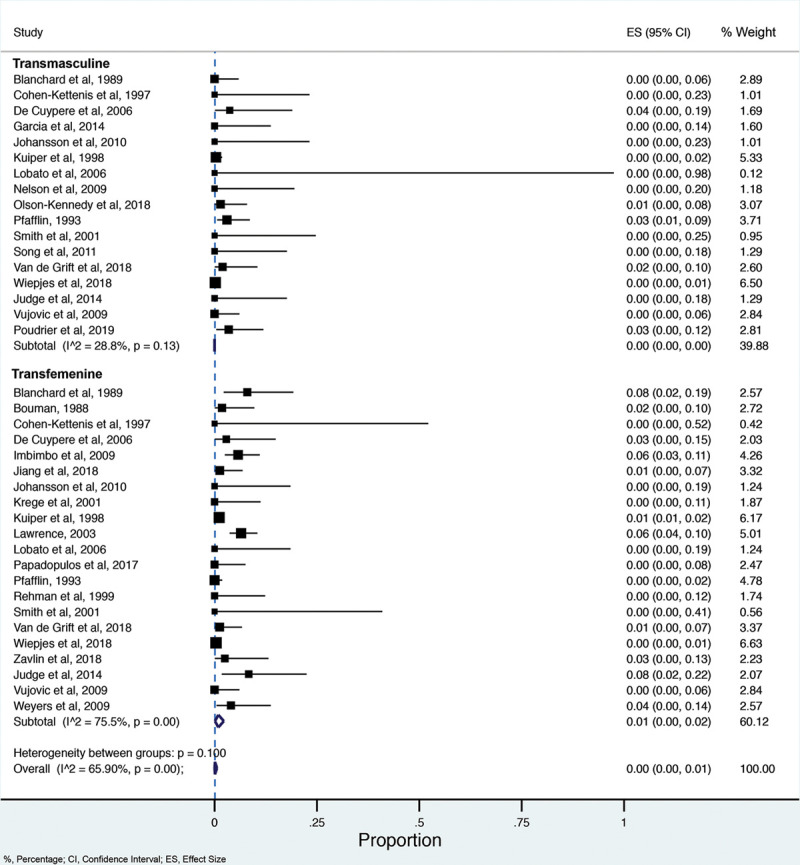
Subgroup analysis of the prevalence of regret among TGNB individuals after gender confirmation surgery based on gender. ES, effect size.
Fig. 4.
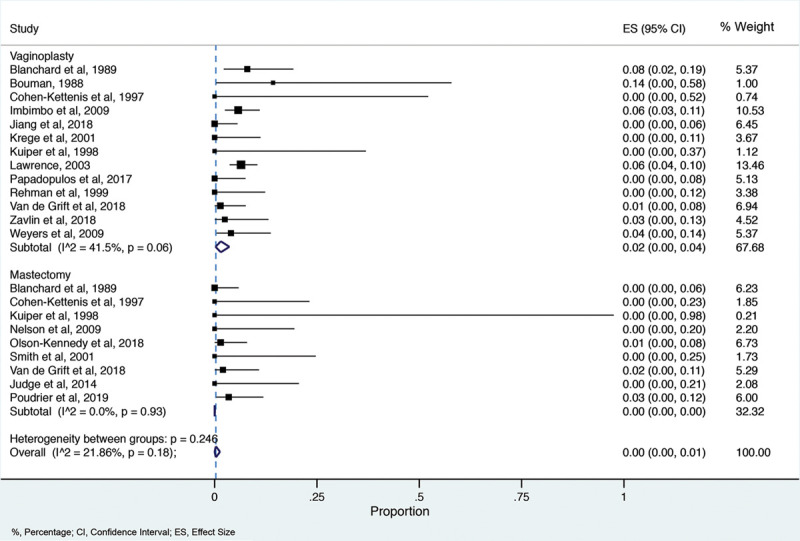
Subgroup analysis of the prevalence of regret among TGNB individuals after gender confirmation surgery based on the type of surgery. ES, effect size.
Meta-regression and Publication Bias
No covariates analyzed affected the pooled endpoint in this metanalysis. The Funnel Plot shows asymmetry between studies (Fig. 5). The Egger test resulted in a P value of 0.0271, which suggests statistical significance for publication bias. The Trim & Fill method imputed 14 approximated studies, with limited impact of the adjusted results. The change in effect size was from 0.010 to 0.005 with no statistical significance (Fig. 6).
Fig. 5.
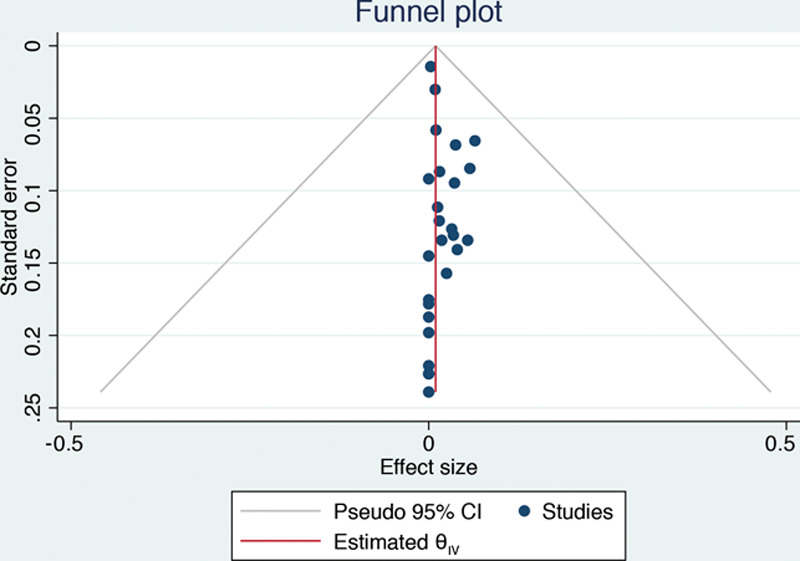
Funnel plot.
Fig. 6.
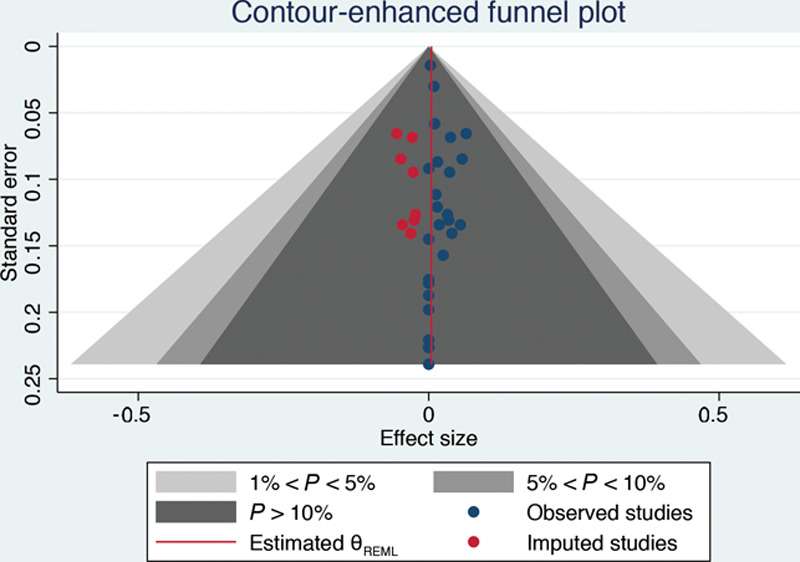
Funnel plot of the Trim & Fill method.
Sensitivity Analysis
When excluding studies with sample sizes less than 10 and high-risk biased studies, the pooled prevalence was similar 1% (CI <1%–3%) compared with the pooled prevalence when those studies were included 1% (CI <1%–2%).
Discussion
The prevalence of regret in the TGNB population after GAS was of 1% (CI <1%–2%). The prevalence of regret for transfemenine surgeries was 1% (CI <1%–2%), and the prevalence for transmasculine surgeries was <1% (CI <1%–<1%). Traditionally, the landmark reference of regret prevalence after GAS has been based on the study by Pfäfflin in 1993, who reported a regret rate of 1%–1.5%. In this study, the author estimated the regret prevalence by analyzing two sources: studies from the previous 30 years in the medical literature and the author’s own clinical practice.20 In the former, the author compiled a total of approximately 1000–1600 transfemenine, and 400–550 transmasculine. In the latter, the author included a total of 196 transfemenine, and 99 transmasculine patients.20 In 1998, Kuiper et al followed 1100 transgender subjects that underwent GAS using social media and snowball sampling.23 Ten experienced regret (9 transmasculine and 1 transfemenine). The overall prevalence of regret after GAS in this study was of 0.9%, and 3% for transmasculine and <0.12% for transfemenine.23 Because these studies were conducted several years ago and were limited to specific countries, these estimations may not be generalizable to the entire TGNB population. However, a clear trend towards low prevalences of regret can be appreciated.
The causes and types of regrets reported in the studies are specified and shown in Table 5 and 6. Overall, the most common reason for regret was psychosocial circumstances, particularly due to difficulties generated by return to society with the new gender in both social and family enviroments.23,29,32,33,36,44 In fact, some patients opted to reverse their gender role to achieve social acceptance, receive better salaries, and preserve relatives and friends relationships. These findings are in line with other studies. Laden et al performed a logistic regression analysis to assess potential risk factors for regret in this population.46 They found that the two most important risk factors predicting regret were “poor support from the family” and “belonging to the non-core group of transsexuals.”46 In addition, a study in Italy hypothesized that the high percentage of regret was attributed to social experience when they return after the surgery.33
Another factor associated with regret (although less prevalent) was poor surgical outcomes.20,23,36 Loss of clitoral sensation and postoperative chronic abdominal pain were the most common reported factors associated with surgical outcomes.14,36 In addition, aesthetic outcomes played an important role in regret. Two studies mentioned concerns with aesthetic outcomes.14,47 Only one of them quoted a patient inconformity: “body doesn’t meet the feminine ideal.”14 Interestingly, Lawrence et al demonstrated in their study that physical results of surgery are by far the most influential in determining satisfaction or regret after GAS than any preoperative factor.36 Concordantly, previous studies have shown absence of regret if sensation in clitoris and vaginal is achieved and if satisfaction with vaginal width is present.36
Other factors associated to regret were identified. Blanchard et al in 1989 noted a strong positive correlation between heterosexual preference and postoperative regret.32 All patients in this study who experienced regret were heterosexual transmen.32 On the contrary, Lawrence et al in 2003 did not find such correlation and attributed their findings to the increase in social tolerance in North American and Western European societies.36 Bodlund et al found that clinically evident personality disorder was a negative prognostic factor for regret in patients undergoing GAS.48 On the other hand, Blanchard et al did not find a correlation among patient’s education, age at surgery, and gender assigned at birth.32
In the present review, nearly half of the patients experienced major regret (based on Pfäfflin classification), meaning that they underwent or desire de-transition surgery, that will never pass through the same process again, and/or experience increase of gender dysphoria from the new gender. One study found that 10 of 14 patients with regret underwent de-transition surgeries (8 mastectomies, 2 vaginectomies, 2 phalloplasties, 2 testicular implants removal, and 1 breast augmentation) for reasons of social regret, true regret or feeling non-binary.23 On the other hand, based on the Kuiper and Cohen Kettenis’ classification, half of the patients in this review had clear regret and uncertain regret. This means that they freely expressed their regret toward the procedure, but some had role reversal to the former gender and others did not. Interestingly, Pfäfflin concluded that from a clinical standpoint, trangender patients suffered from many forms of minor regrets after GAS, all of which have a temporary course.20 This is an important consideration meaning that the actual true regret rate will always remain uncertain, as temporarity and types of regret can bring a huge challenge for assessment.
Regret after GAS may result from the ongoing discrimination that afflicts the TGNB population, affecting their freely expression of gender identity and, consequently feeling regretful from having had surgery.15 Poor social and group support, late-onset gender transition, poor sexual functioning, and mental health problems are factors associated with regret.15 Hence, assessing all these potential factors preoperatively and controlling them if possible could reduce regret rates even more and increase postoperative patient satisfaction.
Regarding transfemenine surgery, vaginoplasty was the most prevalent.14, 19, 23, 30–33, 35, 36, 44, 45Interesintgly, regret rates were higher in vaginoplasties.14,36,44 In this study, we estimated that the overall prevalence of regret after vaginoplasty was 2% (from 11 studies reviewed). This result is slightly higher than a metanalysis of 9 studies from 2017 that reported a prevalence of 1%.13 Moreover, vaginoplasty has shown to increase the quality of life in these patients.13 Mastectomy was the most prevalent transmasculine surgery. Also, it showed a very low prevalence of regret after mastectomy (<1%). Olson-Kennedy et al demonstrated that chest surgery decreases chest dysphoria in both minors and young adults, which might be the major reason behind our findings.38
In the current study, we identified a total of 7928 cases from 14 different countries. To the best of our knowledge, this is the largest attempt to compile the information on regret rates in this population. However, limitations such as significant heterogeneity among studies and among instruments used to assess regret rates, and moderate-to-high risk of bias in some studies represent a big barrier for generalization of the results of this study. The lack of validated questionnaires to evaluate regret in this population is a significant limiting factor. In addition, bias can occur because patients might restrain from expressing regrets due to fear of being judged by the interviewer. Moreover, the temporarity of the feeling of regret in some patients and the variable definition of regret may underestimate the real prevalence of “true” regret.
Based on this meta-analysis, the prevalence of regret is 1%. We believe this reflects and corroborates the increased in accuracy of patient selection criteria for GAS. Efforts should be directed toward the individualization of the patient based on their goals and identification of risk factors for regrets. Surgeons should continue to rigorously follow the current Standard of Care guidelines of the World Professional Association for Transgender Health (WATH).49
CONCLUSIONS
Our study has shown a very low percentage of regret in TGNB population after GAS. We consider that this is a reflection on the improvements in the selection criteria for surgery. However, further studies should be conducted to assess types of regret as well as association with different types of surgical procedure.
Acknowledgments
All the authors have completed the ICMJE uniform disclosure form. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Supplementary Material
Footnotes
Published online 19 March 2021
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Related Digital Media are available in the full-text version of the article on www.PRSGlobalOpen.com.
References
- 1.Safer JD, Tangpricha V. Care of transgender persons. N Engl J Med. 2019; 381:2451–2460 [DOI] [PubMed] [Google Scholar]
- 2.Schechter LS. Gender confirmation surgery: an update for the primary care provider. Transgend Health. 2016; 1:32–40 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Schechter LS. Schechter LS. Background. Surgical Management of the Transgender Patient. 2016, Philadelphia, Pa: Elsevier; 3–7 [Google Scholar]
- 4.Carmel TC, Erickson-Schroth L. Mental health and the transgender population. Psychiatr Ann. 2016; 46:346–349 [DOI] [PubMed] [Google Scholar]
- 5.Wernick JA, Busa S, Matouk K, et al. A systematic review of the psychological benefits of gender-affirming surgery. Urol Clin North Am. 2019; 46:475–486 [DOI] [PubMed] [Google Scholar]
- 6.Flores A R, Brown, et al. How many adults identify as transgender in the United States. The Williams Institute. 2016. (June):15. Available at https://williamsinstitute.law.ucla.edu/publications/trans-adults-united-states/ Accessed June 15, 2020.
- 7.Downing JM, Przedworski JM. Health of transgender adults in the U.S., 2014–2016. Am J Prev Med. 2018; 55:336–344 [DOI] [PubMed] [Google Scholar]
- 8.Lane M, Ives GC, Sluiter EC, et al. Trends in gender-affirming surgery in insured patients in the United States. Plast Reconstr Surg Glob Open. 2018; 6:e1738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nolan IT, Dy GW, Levitt N. Considerations in gender-affirming surgery: demographic trends. Urol Clin North Am. 2019; 46:459–465 [DOI] [PubMed] [Google Scholar]
- 10.Rider GN, Mcmorris BJ, Gower AL, et al. Health and care utilization of transgender and gender nonconforming youth: a population-based study. www.aappublications.org/news. Accessed May 12, 2020 [DOI] [PMC free article] [PubMed]
- 11.American Society of Plastic Surgeons 2018. Plastic Surgery Statistics Report 2018
- 12.American Society of Plastic Surgeons Plastic Surgery Statistics Report 2017. www.plasticsurgery.org. Accessed May 28, 2020
- 13.Manrique OJ, Adabi K, Martinez-Jorge J, et al. Complications and patient-reported outcomes in male-to-female vaginoplasty-where we are today: a systematic review and meta-analysis. Ann Plast Surg. 2018; 80:684–691 [DOI] [PubMed] [Google Scholar]
- 14.van de Grift TC, Elaut E, Cerwenka SC, et al. Surgical satisfaction, quality of life, and their association after gender-affirming surgery: a follow-up study. J Sex Marital Ther. 2018; 44:138–148 [DOI] [PubMed] [Google Scholar]
- 15.Hadj-Moussa M, Ohl DA, Kuzon WM. Feminizing genital gender-confirmation surgery. Sex Med Rev. 2018; 6:457–468.e2 [DOI] [PubMed] [Google Scholar]
- 16.Barone M, Cogliandro A, Di Stefano N, et al. A systematic review of patient-reported outcome measures following transsexual surgery. Aesthetic Plast Surg. 2017; 41:700–713 [DOI] [PubMed] [Google Scholar]
- 17.Agarwal CA, Scheefer MF, Wright LN, et al. Quality of life improvement after chest wall masculinization in female-to-male transgender patients: a prospective study using the BREAST-Q and body uneasiness test. J Plast Reconstr Aesthet Surg. 2018; 71:651–657 [DOI] [PubMed] [Google Scholar]
- 18.Nelson L, Whallett EJ, McGregor JC. Transgender patient satisfaction following reduction mammaplasty. J Plast Reconstr Aesthet Surg. 2009; 62:331–334 [DOI] [PubMed] [Google Scholar]
- 19.Papadopulos NA, Lellé JD, Zavlin D, et al. Quality of life and patient satisfaction following male-to-female sex reassignment surgery. J Sex Med. 2017; 14:721–730 [DOI] [PubMed] [Google Scholar]
- 20.Pfäfflin F. Regrets after sex reassignment surgery. J Psychol Hum Sex. 1993; 5:69–85 [Google Scholar]
- 21.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009; 6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Covidence. Better systematic review management. https://www.covidence.org/home. Accessed May 28, 2020.
- 23.Kuiper AJ, Cohen-Kettenis PT. Gender role reversal among postoperative transsexuals. Int J Transgenderism. 1998; 2 [Google Scholar]
- 24.NIH Study Quality Assessment Tools. Bethesda, Md: National Heart, Lung, and Blood Institute (NHLBI). https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. Accessed May 25, 2020 [Google Scholar]
- 25.Nyaga VN, Arbyn M, Aerts M. Metaprop: a Stata command to perform meta-analysis of binomial data. Arch Public Health. 2014; 72:39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Freeman MF, Tukey JW. Transformations related to the angular and the square root. Ann Math Stat. 1950; 21:607–611 [Google Scholar]
- 27.Rehman J, Lazer S, Benet AE, et al. The reported sex and surgery satisfactions of 28 postoperative male-to-female transsexual patients. Arch Sex Behav. 1999; 28:71–89 [DOI] [PubMed] [Google Scholar]
- 28.Song C, Wong M, Wong CH, et al. Modifications of the radial forearm flap phalloplasty for female-to-male gender reassignment. J Reconstr Microsurg. 2011; 27:115–120 [DOI] [PubMed] [Google Scholar]
- 29.Wiepjes CM, Nota NM, de Blok CJM, et al. The Amsterdam cohort of gender dysphoria study (1972–2015): trends in prevalence, treatment, and regrets. J Sex Med. 2018; 15:582–590 [DOI] [PubMed] [Google Scholar]
- 30.Zavlin D, Schaff J, Lellé JD, et al. Male-to-female sex reassignment surgery using the combined vaginoplasty technique: satisfaction of transgender patients with aesthetic, functional, and sexual outcomes. Aesthetic Plast Surg. 2018; 42:178–187 [DOI] [PubMed] [Google Scholar]
- 31.Weyers S, Elaut E, De Sutter P, et al. Long-term assessment of the physical, mental, and sexual health among transsexual women. J Sex Med. 2009; 6:752–760 [DOI] [PubMed] [Google Scholar]
- 32.Blanchard R, Steiner BW, Clemmensen LH, et al. Prediction of regrets in postoperative transsexuals. Can J Psychiatry. 1989; 34:43–45 [DOI] [PubMed] [Google Scholar]
- 33.Imbimbo C, Verze P, Palmieri A, et al. ORIGINAL RESEARCH-INTERSEX AND GENDER IDENTITY DISORDERS. A report from a single institute’s 14-year experience in treatment of male-to-female transsexuals. J Sex Med. 2009; 6:2736–2745 [DOI] [PubMed] [Google Scholar]
- 34.Johansson A, Sundbom E, Höjerback T, et al. A five-year follow-up study of Swedish adults with gender identity disorder. Arch Sex Behav. 2010; 39:1429–1437 [DOI] [PubMed] [Google Scholar]
- 35.Krege S, Bex A, Lümmen G, et al. Male-to-female transsexualism: a technique, results and long-term follow-up in 66 patients. BJU Int. 2001; 88:396–402 [DOI] [PubMed] [Google Scholar]
- 36.Lawrence AA. Factors associated with satisfaction or regret following male-to-female sex reassignment surgery. Arch Sex Behav. 2003; 32:299–315 [DOI] [PubMed] [Google Scholar]
- 37.Lobato MI, Koff WJ, Manenti C, et al. Follow-up of sex reassignment surgery in transsexuals: a Brazilian cohort. Arch Sex Behav. 2006; 35:711–715 [DOI] [PubMed] [Google Scholar]
- 38.Olson-Kennedy J, Warus J, Okonta V, et al. Chest reconstruction and chest dysphoria in transmasculine minors and young adults: comparisons of nonsurgical and postsurgical cohorts. JAMA Pediatr. 2018; 172:431–436 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Cohen-Kettenis PT, van Goozen SH. Sex reassignment of adolescent transsexuals: a follow-up study. J Am Acad Child Adolesc Psychiatry. 1997; 36:263–271 [DOI] [PubMed] [Google Scholar]
- 40.De Cuypere G, Elaut E, Heylens G, et al. Long-term follow-up: psychosocial outcome of Belgian transsexuals after sex reassignment surgery. Sexologies. 2006; 15:126–133 [Google Scholar]
- 41.Garcia MM, Christopher NA, De Luca F, et al. Overall satisfaction, sexual function, and the durability of neophallus dimensions following staged female to male genital gender confirming surgery: the Institute of Urology, London U.K. experience. Transl Androl Urol. 2014; 3:156–162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Smith YLS, Van Goozen SHM, Cohen-Kettenis PT. Adolescents with gender identity disorder who were accepted or rejected for sex reassignment surgery: a prospective follow-up study. J Am Acad Child Adolesc Psychiatry. 2001; 40:472–481 [DOI] [PubMed] [Google Scholar]
- 43.Judge C, O’Donovan C, Callaghan G, et al. Gender dysphoria – prevalence and co-morbidities in an Irish adult population. Front Endocrinol (Lausanne). 2014; 5:87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Bouman FG. Sex reassignment surgery in male to female transsexuals. Ann Plast Surg. 1988; 21:526–531 [DOI] [PubMed] [Google Scholar]
- 45.Jiang D, Witten J, Berli J, et al. Does depth matter? Factors affecting choice of vulvoplasty over vaginoplasty as gender-affirming genital surgery for transgender women. J Sex Med. 2018; 15:902–906 [DOI] [PubMed] [Google Scholar]
- 46.Landén M, Wålinder J, Hambert G, et al. Factors predictive of regret in sex reassignment. Acta Psychiatr Scand. 1998; 97:284–289 [DOI] [PubMed] [Google Scholar]
- 47.Poudrier G, Nolan IT, Cook TE, et al. Assessing quality of life and patient-reported satisfaction with masculinizing top surgery: a mixed-methods descriptive survey study. Plast Reconstr Surg. 2019; 143:272–279 [DOI] [PubMed] [Google Scholar]
- 48.Bodlund O, Kullgren G. Transsexualism–general outcome and prognostic factors: a five-year follow-up study of nineteen transsexuals in the process of changing sex. Arch Sex Behav. 1996; 25:303–316 [DOI] [PubMed] [Google Scholar]
- 49.Coleman E, Bockting W, Botzer M, et al. Standards of care for the health of transsexual, transgender, and gender-nonconforming people. www.wpath.org. Accessed May 13, 2020
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.