
Fig. 8—
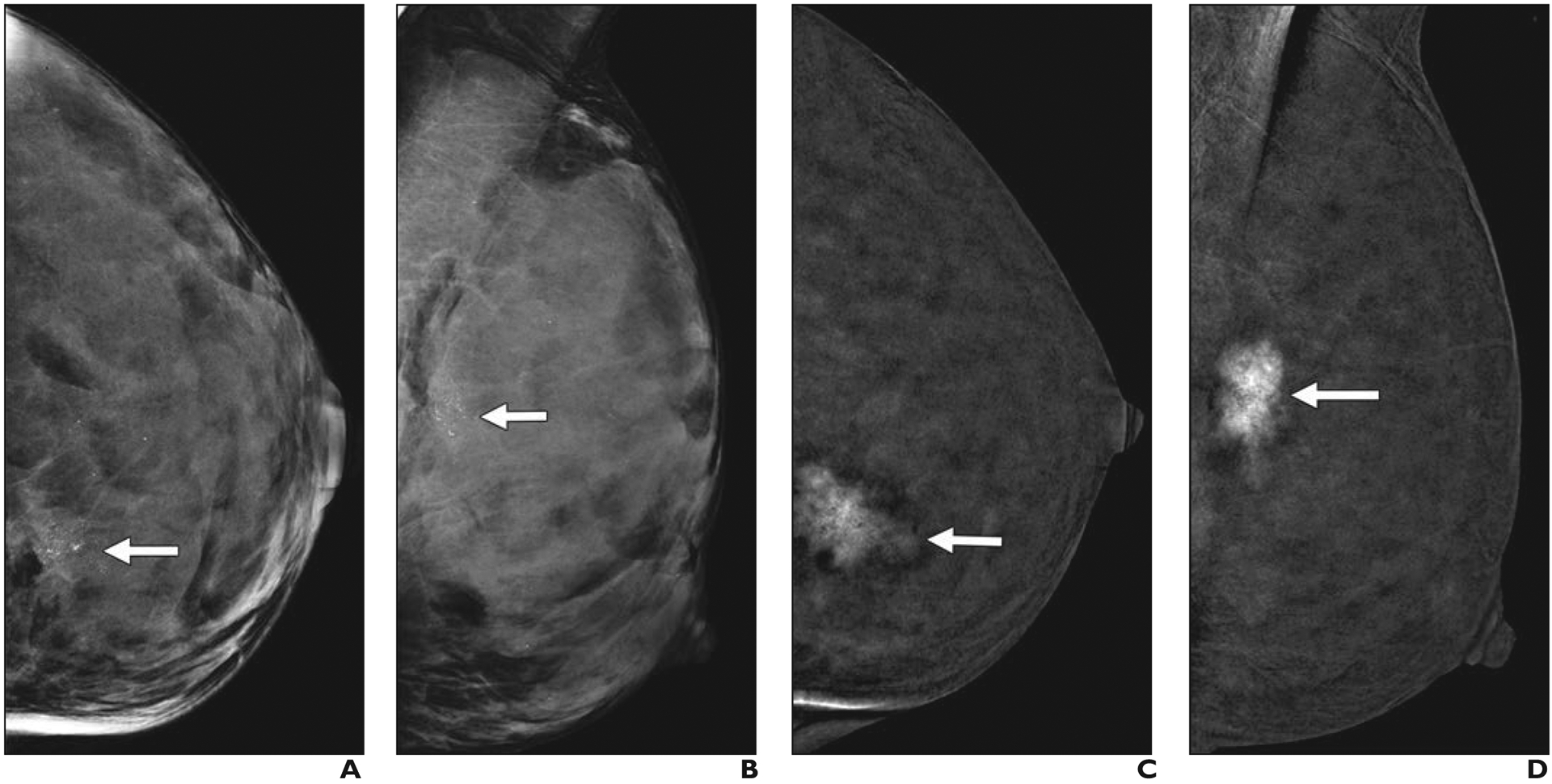
51-year-old woman with extremely dense breasts who had invasive ductal carcinoma visualized using multiple modalities.
A and B, Screening craniocaudal (A) and mediolateral oblique (B) mammography images of left breast show regional amorphous and pleomorphic calcifications (arrows) that are well seen despite extremely dense parenchyma.
C and D, Subtracted craniocaudal (C) and mediolateral oblique (D) images from research contrast-enhanced mammography performed after IV injection of 125 mL of 300 mg I/mL iohexol (Omnipaque 300, GE Healthcare) show strong enhancement of irregular 2.7-cm mass (arrows) at site of calcifications.
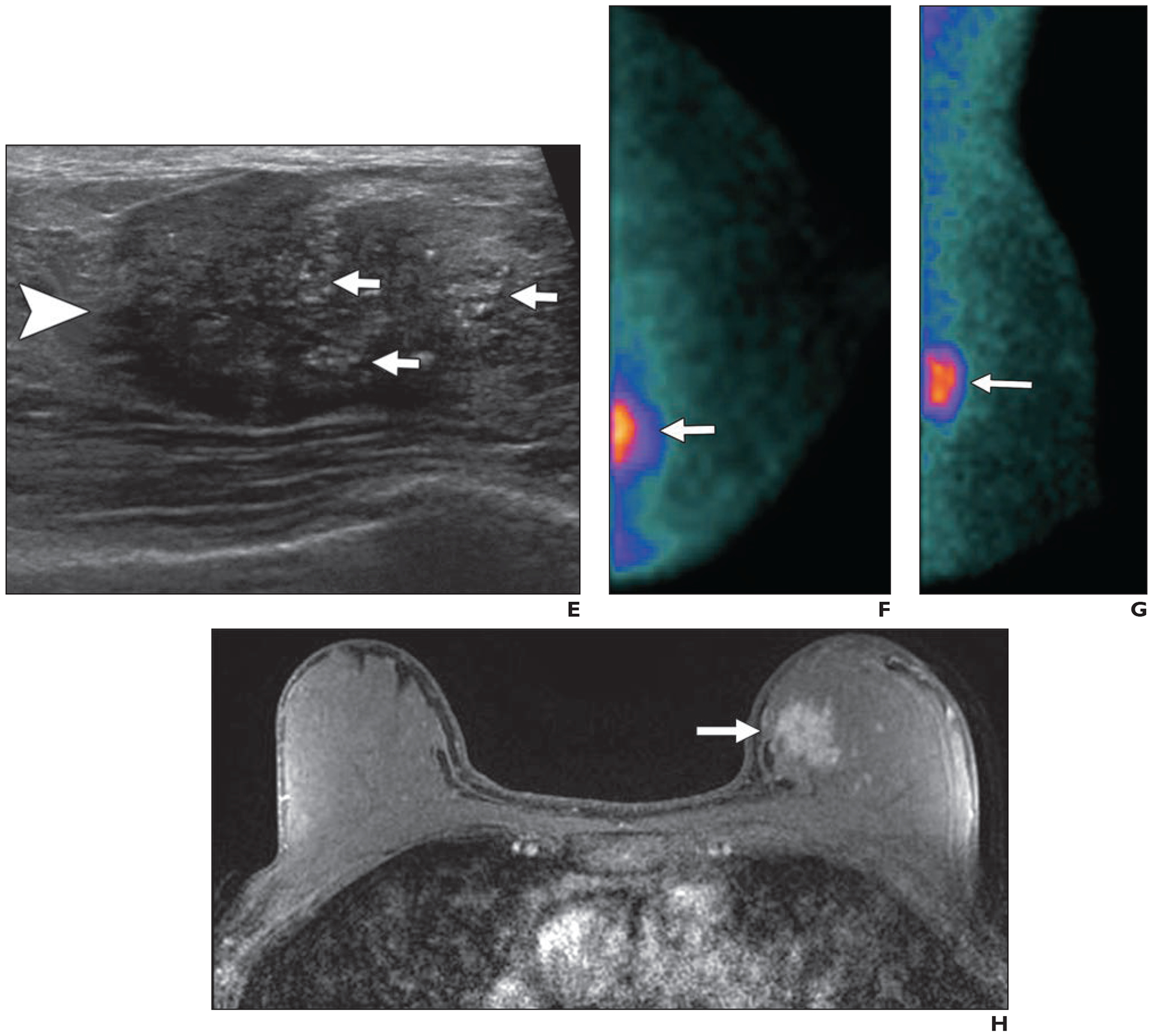
E, Targeted ultrasound image shows partially circumscribed, partially indistinctly marginated, slightly hypoechoic 3.1-cm mass (arrowhead) with echogenic calcifications (arrows). Stereotactic biopsy was performed to ensure optimal sampling of calcifications and showed grade 2 invasive ductal carcinoma with ductal carcinoma in situ that was estrogen receptor negative, progesterone receptor negative, and human epidermal growth factor receptor 2 (HER2 [also known as ERBB2]) negative. Ki-67 proliferation index was low (10%).
F and G, Craniocaudal (F) and mediolateral oblique (G) views from research molecular breast imaging (10-minute acquisitions obtained after IV injection of 7.3 mCi [270.1 MBq] of 99mTc-sestamibi) performed after diagnosis shows intense uptake in irregular 3.4-cm mass (arrows). Note slight reduction in inclusion of extreme posterior tissues relative to mammography.
H, Axial fat-suppressed T1-weighted MR image shows intense enhancement of irregular 3.0-cm mass (arrow) at site of known malignancy. Patient had partial response to primary chemotherapy with two sentinel nodes negative for metastases (or therapy-related changes).