

Abstract
Objective
To identify health states that patients with acute stroke deem worse than death and to explore potential predictors for these ratings.
Methods
This was a cross-sectional study involving patients admitted to an urban comprehensive stroke center with acute stroke. Participants were asked to rate 10 possible health states/functional outcomes as better or worse than death using a 5-point Likert scale. Principal component analysis (PCA) was used to reduce clusters of correlated ratings to summary components (factors). These components were then analyzed using linear regression to identify possible predictive variables.
Results
Eighty patients participated. The states deemed equal to or worse than death by the majority of participants were relying on a breathing machine (66%) or feeding tube (66%), persistent confusion (62%), inability to communicate with others (58%), and bowel/bladder incontinence (50%). PCA revealed 2 factors of correlated variables: factor 1 composed primarily of relying on a feeding tube or breathing machine, incontinence, chronic pain, and persistent confusion, and factor 2 composed primarily of using a wheelchair, being bedbound, living in a nursing home, and requiring help for activities of daily living. The only significant predictor found was race for factor 1, with black participants finding these states more preferable to death than white participants.
Discussion
A substantial number of patients found multiple common outcomes of stroke to be the same as or worse than death. This highlights the importance of realistic discussions about expected functional outcomes with patients and/or their surrogate decision makers when considering goals of care after stroke.
Around 10% of patients with acute stroke will require mechanical ventilation for respiratory failure or airway protection1 and/or have a long-term feeding tube placed.2 Unfortunately, patients with stroke are frequently unable to participate in treatment preference conversations due to aphasia or encephalopathy. Physicians then have to rely on surrogate decision makers to guide treatment decisions, which is fraught with issues due to difficulty with prognostication,3,4 differences between physician and surrogate beliefs on prognosis,5 and lack of advance directives.6 The ultimate goal of surrogate decision making is to make treatment decisions based on the patient's known or assumed wishes,7 but this standard is frequently not met in actual practice.8 Physicians may struggle with how to elicit patients' values and beliefs and integrate these into goals-of-care conversations.
The objective of this study was to assess what health states patients with acute stroke consider worse than death and determine whether there are any predictors for these ratings.
Patient attitudes about negative health states were previously studied in patients with advanced cancer, congestive heart failure, and lung disease by asking them to rate 10 possible health states/outcomes relative to death.9 Given the differences between these chronic, progressive conditions and the acute changes of stroke with potential for recovery, there is reason to believe that patients with stroke may rate these possible outcomes differently. Knowledge of what states patients with stroke consider worse than death could help physicians to elicit preferences and decide on treatments by providing “talking points” during goals-of-care conversations. The objective of this study was to assess what health states patients with acute stroke consider worse than death and determine whether there are any predictors for these ratings.
Methods
This was a cross-sectional study of patients admitted to a comprehensive stroke center in an urban Midwest setting between September 2017 and April 2019. Convenience sampling was used. Inclusion criteria were age ≥18 years, English speaking, and admitted to the stroke service with a diagnosis of acute stroke (ischemic or hemorrhagic). Exclusion criteria were a diagnosis of an active malignancy or a condition that would render the patient unable to understand the questionnaire (e.g., advanced dementia and aphasia).
Each participant was provided with a questionnaire to separately rank 10 health states or functional outcomes on a 5-point Likert scale consisting of “much better than death,” “somewhat better than death,” “little bit better than death,” “neither better nor worse than death,” or “worse than death.” The chosen health states and rankings were based on a previous study9 with an added state of “being unable to communicate,” as this is a common and devastating stroke deficit. Basic demographic data were collected from the participant (age, sex, race [self-identified, multiple selections were allowed], education, marital status, prestroke modified Rankin Scale, and prestroke self-health rating), and the Short Blessed Test (SBT) was performed to assess cognitive function.10
The primary analytics question addressed in this study was whether demographic features of an individual patient predict their responses to the Likert scale rating questions. The dependent variables for the analysis were initially the ratings to the 10 questions; however, there was a strong correlation among responses across individuals. As a result, these data encoded many fewer “dimensions” or “components” than 10. It is well established that highly correlated variables can be reduced or summarized into components that represent weighted averages of the original variables.11 The simplest method most suited for this task is principal component analysis (PCA). This approach is commonly used to behavioral analysis12 and accomplishes 2 important tasks: first, it identifies a smaller number of latent components that well explain the original data, and second, the resulting components are by definition not correlated (independent), which meets the assumption of many statistical tests.
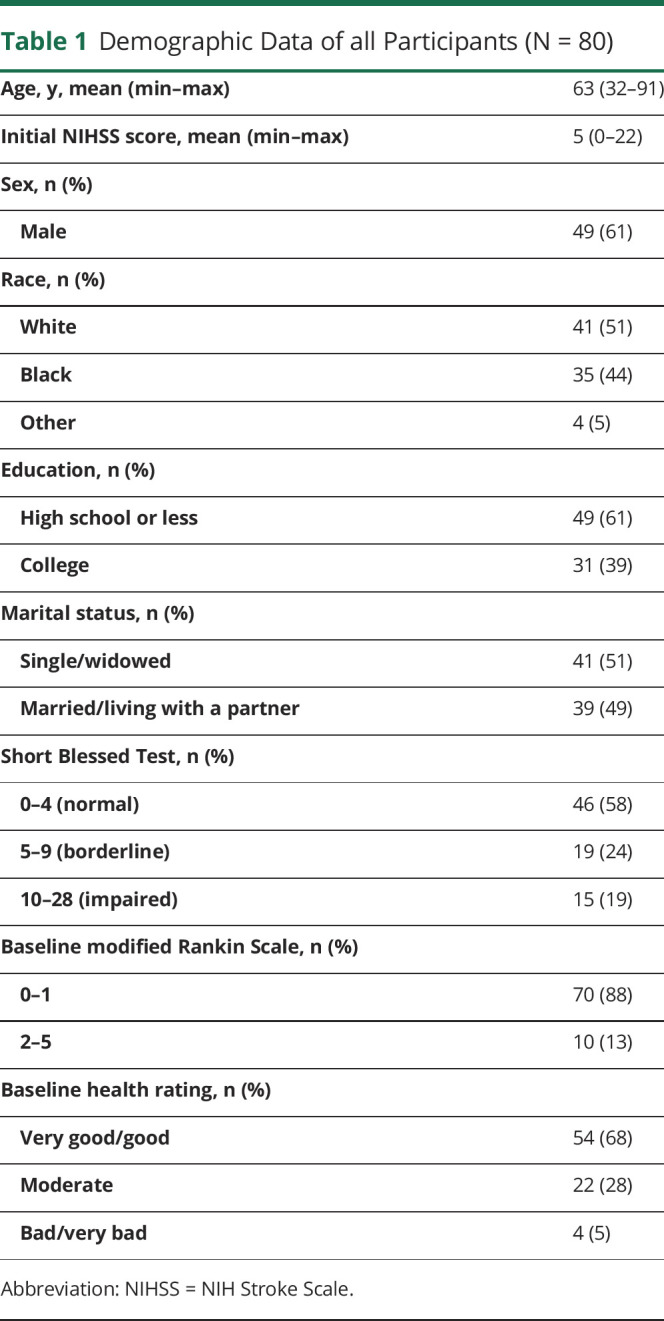
PCA results in components (also called factors) defined with “factor loadings,” which describe how strongly each original variable (in this case, question rating) contributes to that component.11 A factor score is then assigned to each participant for each identified component; this represents the weighted average of their ratings. These factor scores were then subjected to linear regression to identify demographic variables that could predict ratings. Included potential predictors were age, sex, race, education level, marital status, and initial NIH Stroke Scale (NIHSS) score; groupings for these variables were used as seen in table 1. The backward stepwise method was used, with the exclusion criteria being a p < 0.05 for the potential predictor's significance. Statistical analysis was performed using SPSS Statistics, version 25.0 (IBM, Armonk, NY).
Table 1.
Demographic Data of all Participants (N = 80)
Standard Protocol Approvals, Registrations, and Patient Consents
The Institutional Review Board at Washington University in St. Louis approved the study protocol. All participants provided written informed consent.
Data Availability
Anonymized data not provided in the article will be shared at the request of any qualified investigator.
Results
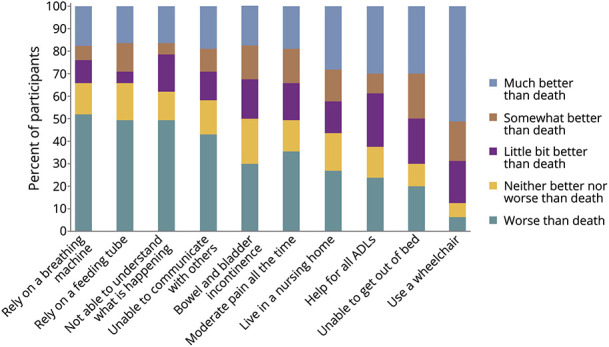
A total of 347 patients were screened for eligibility, and 149 patients met the criteria. Thirty-two eligible patients refused to participate, 37 patients were off the floor for testing when approached, and 80 total patients participated in the study. Demographic information for participants is shown in table 1. The initial documented NIHSS score for each participant had a mean of 5, with 25% of participants having an NIHSS score of 9 or greater. The figure illustrates the distribution of ratings for all queried health states. Ratings widely varied across individuals, but 50% or more of participants deemed requiring a breathing machine or feeding tube to live, being confused all of the time, being unable to communicate, and bowel and bladder incontinence as “neither better nor worse” or “worse than death.” The least objectionable state was needing to use a wheelchair, with only 13% deeming it as the same as or worse than death. Kendall τ test was used to correlate ratings; ratings within individuals were highly correlated, with the τ ranging from 0.26 to 0.75, p < 0.001 for all.
The least objectionable state was needing to use a wheelchair, with only 13% deeming it as the same as or worse than death.
Figure. Ratings of Select Health States Relative to Death by Patients With Acute Stroke (N = 80).

Distribution of patient ratings on selected health states or functional debilities on a 5-point Likert scale, arranged in declining order of most objectionable (highest rated “neither better nor worse” or “worse than death”) to least. ADLs = activities of daily living.
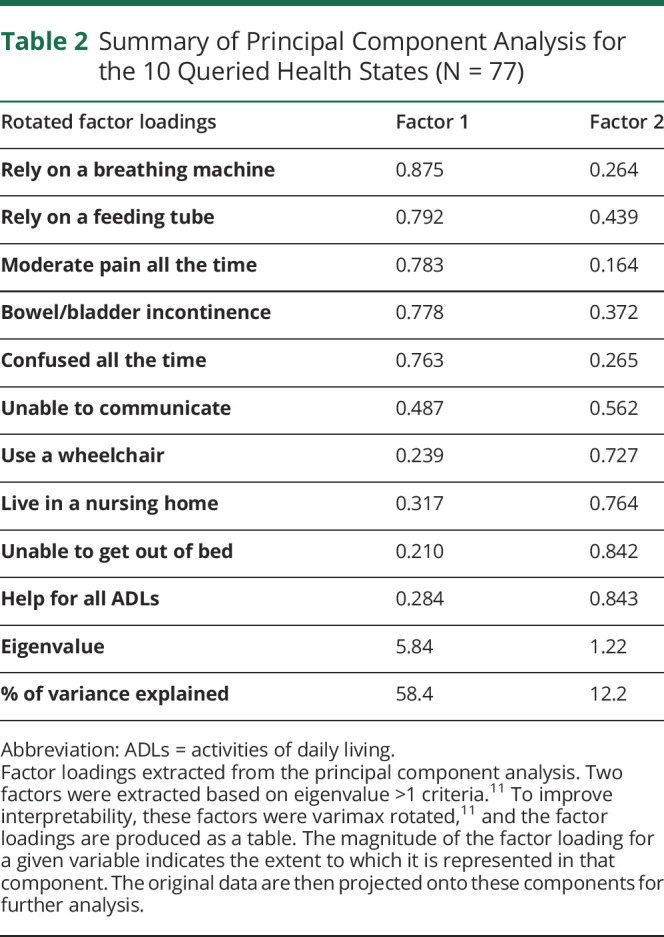
Ratings were then subjected to PCA; complete data were missing for 3 participants, so 77 total cases were used. Sample size adequacy was verified with an overall Kaiser-Meyer-Olkin measure of 0.88. Appropriate correlation size between each participant's ratings was verified with a significant Bartlett test of sphericity. Two components were retained by the criteria that the eigenvalue be greater than 1, a common heuristic approach.11 The fraction of the original variance explained by these 2 factors was 70.6%, which means that 70.6% of the information encoded by the 10 questions is known using this reduced 2-component (dimensional) space. Table 2 shows factor loadings (the weighting of how each question contributes to the component). The states that loaded the most on factor 1 were requiring a breathing machine and feeding tube, being in moderate pain all of the time, bowel/bladder incontinence, and being confused all of the time. The states that loaded the most on factor 2 were using a wheelchair, living in a nursing home, being bedbound, and requiring help for all activities of daily living (ADLs). The identification of these 2 factors implies that individuals differed in their responses along these 2 dimensions (i.e., the answers to the questions in factor 1 are not correlated across participants to the answers to questions in factor 2).
Table 2.
Summary of Principal Component Analysis for the 10 Queried Health States (N = 77)
The 2 identified factors were then subjected to linear regression analysis to evaluate for predictive factors. For factor 1, the only significant predictor identified was race (p = 0.006, β-coefficient −0.321, 95% confidence interval −0.542 to −0.100); the model had an R2 of 0.10. Mean scores were compared for black and white participants; the mean was lower for black participants, indicating that they looked more favorably on the state as being better than death. For factor 2, none of the variables were significant for predicting responses.
Discussion
This study examined how patients with acute stroke felt about possible health states/functional debilities relative to death. As expected, responses were heterogeneous, but the most objectionable states for participants included requiring a breathing machine or feeding tube, being confused all of the time, being unable to communicate with others, and bowel/bladder incontinence. PCA reduced the state ratings to 2 factors: factor 1 was weighted heaviest with the more intensive life-sustaining states (requiring a breathing machine and feeding tube) as well as constant pain and confusion. Factor 2 was weighted heaviest with states related to mobility (using a wheelchair, being bedbound, and living in a nursing home) and requiring help with ADLs. These findings indicate that patients may think of debilities relating to mobility and requiring physical help differently than those that involve life-sustaining treatments or unrelenting, undesirable bodily states (pain, confusion), with the latter states comparable to or worse than dying.
The only demographic value that was predictive of these responses was race for factor 1, which indicated that the black patients looked on the overall most undesirable states more positively than white patients. This conforms with the previous studies, which have demonstrated that black patients are more likely to prefer and receive invasive treatments and intensive hospital care at the end of life.13,14 The reasoning behind this is likely multifactorial, including lack of advance planning documentation,15 use of hospitals with higher intensive care16 and less palliative care17 use, religious beliefs,18 and a distrust of the medical establishment.19 The lack of other easily found predictors (including sex, marital status, education, and initial NIHSS score) is indicative of the fact that patient values and beliefs are extremely individualized and influenced by a great many factors.
The findings in this population are overall comparable to the previous study that involved chronically ill patients,9 with a few notable differences. This stroke population found chronic pain to be much more intolerable (49% rated as the same as or worse than death vs approximately 13%), and bowel/bladder incontinence was less objectionable to them than the chronically ill population (50% vs 69%). This is likely reflective of the fact that the chronically ill population has more chronic pain than this population that was relatively healthy before their stroke; research has demonstrated that people tend to inaccurately predict how a chronic disability will affect their well-being.20 On the contrary, this stroke population has likely had little experience with the stress and embarrassment of bowel/bladder incontinence and requiring help for such a personal ADL, so they may look on it more favorably than those who have dealt with it before. On the whole, however, the clustering of states into those more and less objectionable was retained between the 2 studies despite the acute vs chronic nature of the medical problems, indicating that these groupings may be more generalizable.
Limitations of this study include the sample size, patients being recruited from a single site (though with a wide referral area encompassing both rural and urban populations), and the patients' overall minimal prestroke functional impairments and milder strokes, although many of the patients were at the time of enrollment being faced with some of the states that they were rating, including feeding tube placement, wheelchair use, nursing home placement, and requiring help with ADLs. Findings may not be generalizable to patients with more severe strokes or worse prestroke functional impairment. A number of important possible predictors for ratings were missing from the data, including religiosity/spirituality and socioeconomic status. The cognitive dysfunction of a substantial minority (40%) of the participants as evidenced by SBT scores should be taken into consideration when interpreting results of this self-reported survey, although these patients were deemed to have decision-making capacity by their medical team and were making treatment decisions for themselves at the time of participation.
The results of this study can provide a framework for physicians to approach patients with stroke and their families during discussions about treatment options and goals of care by highlighting the outcomes that are most feared. When attempting to elucidate patient values and preferences from patients or their surrogate decision makers, the outcomes that these participants found the most intolerable (breathing and feeding tubes, constant confusion, and incontinence) can be used to describe potential/predicted future symptom burden and care needs, followed by an exploration of the patient's known or predicted feelings about these outcomes. There are, of course, the caveats that acute symptoms can lessen or resolve over time (thus making feeding tubes or nursing home care unnecessary), and patients can adapt to previously feared disabilities, as evidenced by the “disability paradox,”20 an often-repeated observation that people with severe and persistent disabilities (including those caused by spinal cord injury,21 stroke,22 and amyotrophic lateral sclerosis23) report a better quality of life than external observers expect them to have. This study also emphasizes the very personal nature of these preferences that result from a lifetime of different experiences and cannot be predicted based on baseline demographic factors, meaning physicians must delve carefully into each individual patient's values and beliefs before making these important clinical decisions.
TAKE-HOME POINTS
→ Requiring a breathing machine or feeding tube, being confused all of the time, being unable to communicate, and bowel/bladder incontinence were considered the most objectionable outcomes by patients with acute stroke.
→ Patient demographics were overall not predictive of patients' feelings about negative health outcomes.
→ Evaluation of patient values and beliefs is essential when discussing treatment preferences with patients and families after stroke.
Appendix. Authors
Footnotes
Editorial, page 3
Study Funding
No targeted funding reported.
Disclosure
The authors report no disclosures relevant to the manuscript. Full disclosure form information provided by the authors is available with the full text of this article at Neurology.org/cp.
References
- 1.Lahiri S, Mayer S, Fink M, et al. Mechanical ventilation for acute stroke: a multi-state population-based study. Neurocrit Care 2015;23:28–32. [DOI] [PubMed] [Google Scholar]
- 2.George B, Kelly A, Schneider E, Holloway R. Current practices in feeding tube placement for US acute ischemic stroke inpatients. Neurology 2014;83:874–882. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Persaud N, Thorpe K, Raptis S, Saposnik G. Why clinicians prognosticate stroke patients poorly: results from the clinician judgement versus risk score to predict stroke outcomes randomized study. J Stroke Cerebrovasc Dis 2016;25:1349–1354. [DOI] [PubMed] [Google Scholar]
- 4.Holloway R, Arnold R, Creutzfeldt C, et al. Palliative and end-of-life care in stroke. Stroke 2014;45:1887–1916. [DOI] [PubMed] [Google Scholar]
- 5.White D, Ernecoff N, Buddadhumaruk P, et al. Prevalence of and factors related to discordance about prognosis between physicians and surrogate decision makers of critically ill patients. JAMA 2016;315:2086–2094. [DOI] [PubMed] [Google Scholar]
- 6.Yadav KN, Gabler NB, Cooney E, et al. Approximately one in three US adults completes any type of advance directive for end-of-life care. Health Aff (Millwood) 2017;36:1244–1251. [DOI] [PubMed] [Google Scholar]
- 7.Berger JT, DeRenzo EG, Schwartz J. Surrogate decision making: reconciling ethical theory and clinical practice. Ann Intern Med 2008;149:48–53. [DOI] [PubMed] [Google Scholar]
- 8.Scheunemann LP, Ernecoff NC, Buddadhumaruk P, et al. Clinician-family communication about patients' values and preferences in intensive care units. JAMA Intern Med 2019;179:676–684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rubin E, Buehler A, Halpern S. States worse than death among hospitalized patients with serious illnesses. JAMA Intern Med 2016;176:1557–1559. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Carpenter CR, Bassett ER, Fischer GM, Shirshekan J, Galvin JE, Morris JC. Four sensitive screening tools to detect cognitive dysfunction in geriatric emergency department patients: brief Alzheimer's Screen, Short Blessed Test, Ottawa 3DY, and the caregiver-completed AD8. Acad Emerg Med 2011;18:374–384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Abdi H, Williams LJ. Principal component analysis. WIREs Comp Stats 2010;2:433–459. [Google Scholar]
- 12.Jolliffe IT, Cadima J. Principal component analysis: a review and recent developments. Philos Trans A Math Phys Eng Sci 2016;374:20150202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Barnato AE, Anthony DL, Skinner J, Gallagher PM, Fisher ES. Racial and ethnic differences in preferences for end-of-life treatment. J Gen Intern Med 2009;24:695–701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Singh T, Peters SR, Tirschwell DL, Creutzfeldt CJ. Palliative care for hospitalized patients with stroke: results from the 2010 to 2012 national inpatient sample. Stroke 2017;48:2534–2540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kahana E, Kahana B, Bhatta T, Langendoerfer KB, Lee JE, Lekhak N. Racial differences in future care planning in late life. Ethn Health Epub 2019 Jan 29. doi: 10.1080/13557858.2019.1573974. [DOI] [PubMed]
- 16.Wang SY, Hsu SH, Huang S, Doan KC, Gross CP, Ma X. Regional practice patterns and racial/ethnic differences in intensity of end-of-life care. Health Serv Res 2018;53:4291–4309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Faigle R, Ziai WC, Urrutia VC, Cooper LA, Gottesman RF. Racial differences in palliative care use after stroke in majority-white, minority-serving, and racially integrated US hospitals. Crit Care Med 2017;45:2046–2054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Johnson KS, Elbert-Avila KI, Tulsky JA. The influence of spiritual beliefs and practices on the treatment preferences of African Americans: a review of the literature. J Am Geriatr Soc 2005;53:711–719. [DOI] [PubMed] [Google Scholar]
- 19.Cort MA. Cultural mistrust and use of hospice care: challenges and remedies. J Palliat Med 2004;7:63–71. [DOI] [PubMed] [Google Scholar]
- 20.Ubel PA, Loewenstein G, Schwarz N, Smith D. Misimaging the unimaginable: the disability paradox and health care decision making. Health Psychol 2005;24:S57–S62. [DOI] [PubMed] [Google Scholar]
- 21.Albrecht GL, Devlieger PJ. The disability paradox: high quality of life against all odds. Soc Sci Med 1999;48:977–988. [DOI] [PubMed] [Google Scholar]
- 22.Creutzfeldt C, Holloway R. Treatment decisions after severe stroke: uncertainty and biases. Stroke 2012;43:3405–3408. [DOI] [PubMed] [Google Scholar]
- 23.Kuzma-Kozakiewicz M, Andersen PM, Ciecwierska K, et al. An observational study on quality of life and preferences to sustain life in locked-in state. Neurology 2019;93:e938–e945. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Anonymized data not provided in the article will be shared at the request of any qualified investigator.