
Figure 2.
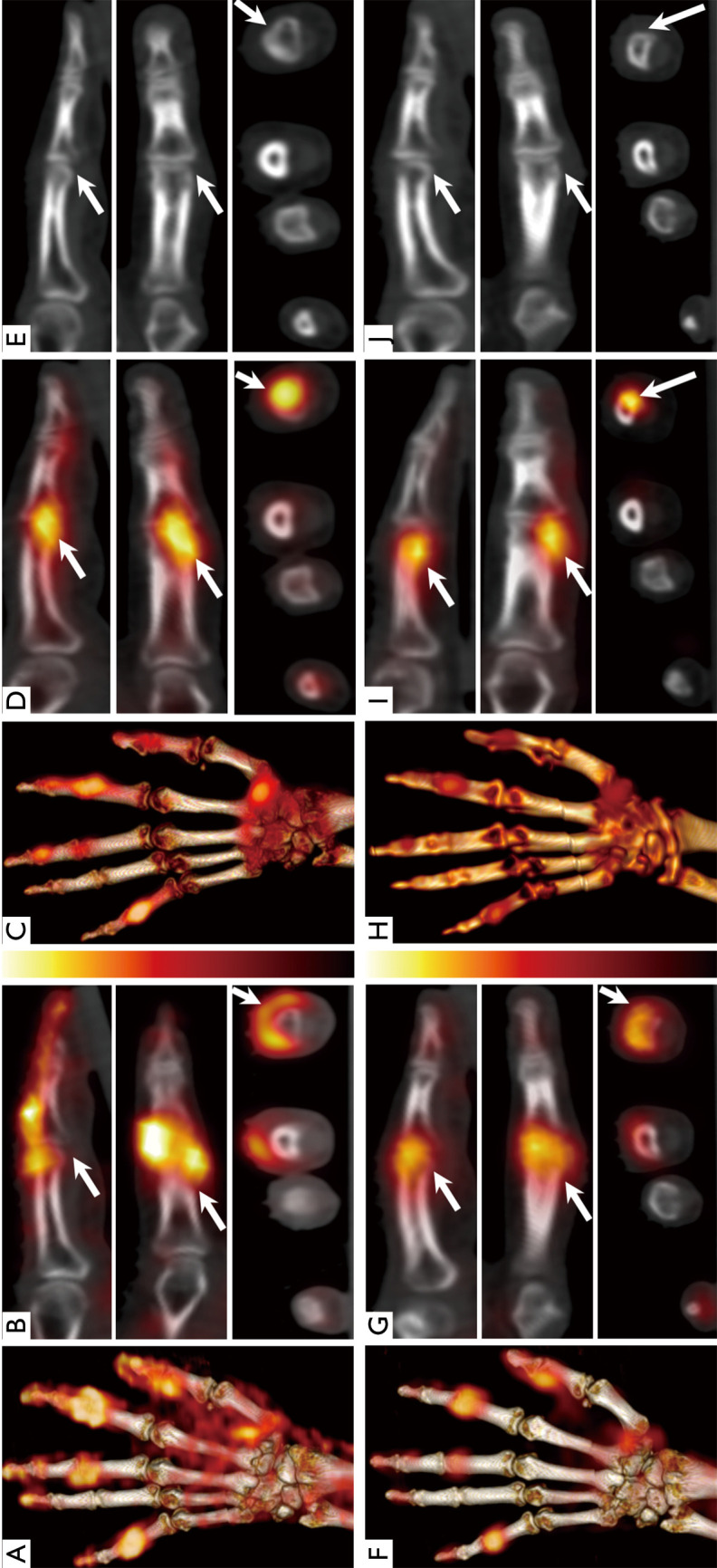
SPECT/CT images of a 74-year-old patient with seropositive RA at the baseline (top; A,B,C,D,E) and one-month (bottom; F,G,H,I,J) after therapy: volume rendered maximum intensity projection (MIP) of the fused SPECT/CT images of the left hand (A C,F,H) and magnified SPECT/CT images of the 2nd finger PIP joint (arrow; B,D,G,I) in sagittal (top), coronal (middle) and axial (bottom) projections, with the corresponding low-dose CT (E,J). Baseline soft-tissue SPECT/CT (A) demonstrates hypervascularity in 1st IP & CMC, 2nd, 3rd & 5th PIP joints, with nearly circumferential hypervascularity pattern around the 2nd PIP (B). Corresponding MIP from the osseous SPECT/CT phase (C) showing increased osseous turnover in the 2nd and 5th PIP regions with asymmetric tracer distribution across the joint. The uptake is more prominent on the radial aspect of the distal end of the proximal phalanx of the 2nd PIP (D). The corresponding low-dose CT images (E) show no evidence of erosive changes. The follow-up images (F-J) demonstrate significant improvement of the previously noted hypervascularity of the affected joints (F). Second PIP joint images (G) demonstrate the most striking changes in tracer intensity and distribution. The osseous phase images (H, I) also demonstrate reduction of tracer uptake, but still eccentric and radially located. There was no clear evidence of erosions on the low-dose CT (J). SPECT/CT, single photon emission computed tomography/computed tomography; RA, rheumatoid arthritis; MIP, maximum intensity projection; PIP, proximal interphalangeal; IP, interphalangeal; CMC, carpo-metacarpal.