
Figure 2.
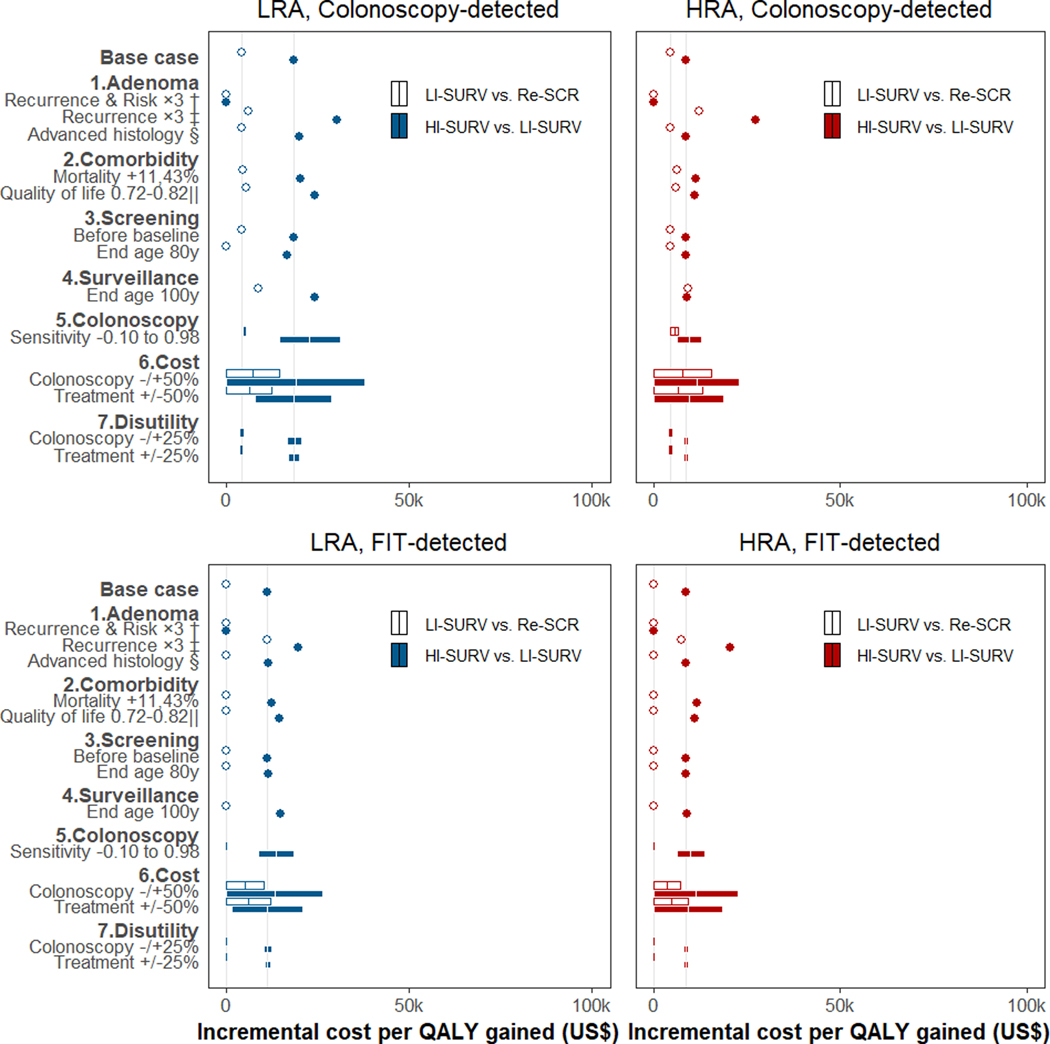
Sensitivity analysis of incremental cost-effectiveness ratios for surveillance in 50-year-old patients with adenoma detected at screening colonoscopy or FIT *
Abbreviations: HI = high-intensity; HRA = high-risk adenoma (≥3 small adenomas or ≥1 large); LI = low-intensity; LRA = low-risk adenoma (1–2 small adenomas); QALY = quality-adjusted life year; Re = return; SCR = screening; SURV = surveillance.
* Incremental cost-effectiveness for low-intensity surveillance scenarios was relative to the scenario of return to routine screening in 10 years; incremental cost-effectiveness for high-intensity surveillance was relative to low-intensity surveillance. Grey vertical lines represent the base-case ratios. Results for persons with adenomas detected by baseline screening at older ages are in Supplementary Figure 11, 13.
† The recurrence of advanced adenoma at surveillance and the associated CRC risk were increased approximately three-fold to better match some of the observed data (Supplementary Figure 6, Panel d; Supplementary Figure 8). The increase was accomplished by decreasing the assumed average time it takes for a new adenoma to become large and develop into cancer.
‡ The recurrence of advanced adenoma was increased three-fold to better match observed data (Supplementary Figure 6, Panel d), but CRC risk was kept consistent with the Surveillance Epidemiology and End Results program data used for model calibration. This was accomplished by decreasing the assumed time for a new polyp to become large, but increasing the subsequent time to cancer.
§ Results for LRA patients were corrected for misclassification of small adenoma with advanced histological features (villous histology or high-grade dysplasia) under the assumption that these lesions behave similar to HRA.
‖ The quality of life for the population was decreased with age to reflect overall deteriorating health with age.(57)