
Figure 1.
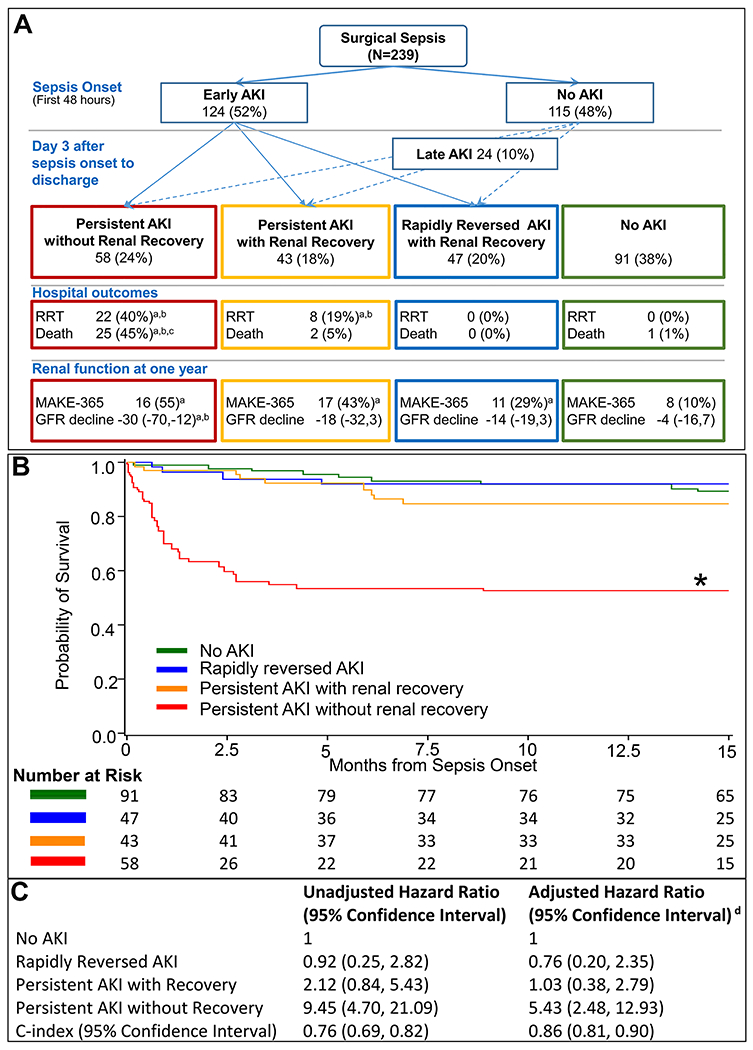
A. Trajectories of acute kidney injury in sepsis
a Significantly different from No AKI group (Bonferroni-adjusted p<0.05)
b Significantly different from rapidly reversed AKI group (Bonferroni-adjusted p<0.05)
c Significantly different from persistent AKI with recovery (Bonferroni-adjusted p<0.05)
B. Adjusted Kaplan-Meier survival curves and number at risk by AKI trajectories Propensity score based inverse weighting was used to plot adjusted Kaplan Meier curves where propensity of being in a trajectory group was calculated using multinomial logistic model that included patient demographics (age, gender, ethnicity), Charlson comorbidity score, septic shock and non-renal SOFA score on sepsis onset.
C. Hazard ratios for all-cause mortality by AKI trajectories
* p<0.05 for Bonferroni-adjusted log-rank test when compared to all other groups
d Adjusted for age, gender, ethnicity, Charlson comorbidity score, sepsis shock status and non-renal SOFA score on sepsis onset, and total ICU length of stay.
Abbreviations. RRT, renal replacement therapy; GFR, glomerular filtration rate ; MAKE-365, major adverse kidney events composite outcome of death, renal replacement therapy dependence, or having an estimated GFR less than 60 ml/min/1.72m2 at one year of sepsis onset. Hospital outcomes were reported among patients who were not withdrawn from the study at the time of hospital discharge and one year outcomes were reported among hospital survivors were not withdrawn from the study and had renal data available at one year.