
Fig. 2—
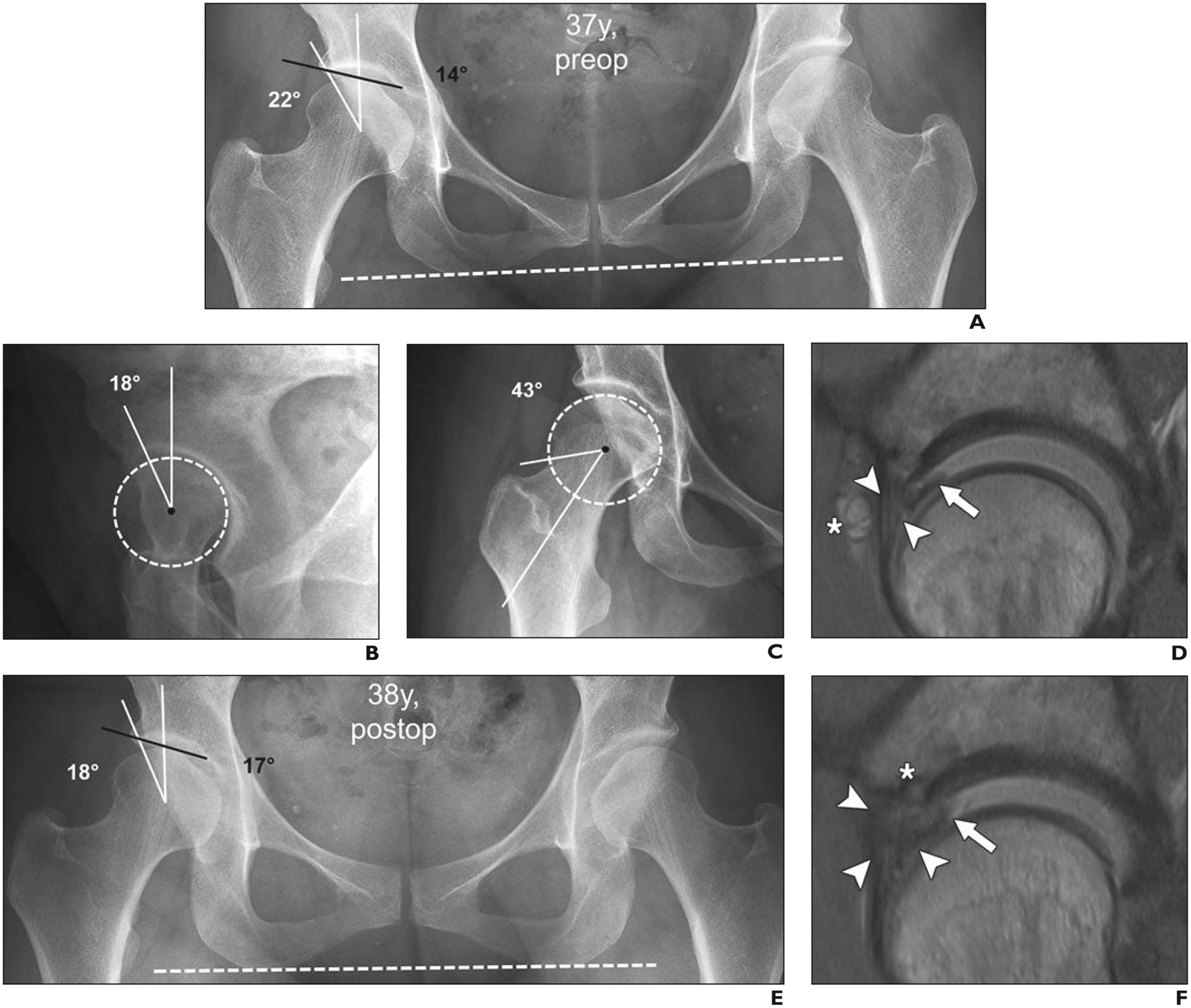
37-year-old woman with right-sided groin pain with prolonged standing and provocative pain with flexion and internal rotation during clinical examination (positive anterior impingement test). This case of incorrect management of developmental dysplasia of hip (DDH) as femoroacetabular impingement (FAI) underlines importance of correct identification of DDH before FAI surgery.
A, Anteroposterior radiograph of pelvis shows preserved joint space and DDH on right (lateral center-edge angle, 22° [white lines]; acetabular index, 14° [black line]). Dashed line indicates anatomic horizontal reference axis.
B, False-profile-view radiograph shows deficient anterior coverage with anterior center-edge angle of 18°. Dashed circle indicates best-fitting circle of femoral head to define femoral rotation center.
C, Forty-five-degree Dunn-view radiograph shows no cam deformity (alpha angle, 43°) at anterosuperior femoral head-neck junction. Dashed circle indicates best-fitting circle of femoral head to define femoral rotation center.
D, Sagittal proton density–weighted image from direct MR arthrogram obtained with application of leg traction shows hypertrophic anterosuperior labrum (arrowheads) with mucoid degeneration and associated paralabral cyst (asterisk) and flap tear (arrow) at chondrolabral junction. Overall, these findings are indicative of hip instability rather than impingement conflict. Patient underwent arthroscopic labral repair with trimming of acetabular rim and reattachment of labrum.
E, Anteroposterior radiograph of pelvis 1 year after arthroscopic labral repair with trimming of acetabular rim and reattachment of labrum shows iatrogenic progression of dysplasia of right hip after acetabuloplasty (lateral center-edge angle, 18° [white lines]; acetabular index, 17° [black line]). Dashed line indicates anatomic horizontal reference axis.
F, Sagittal proton density–weighted MR arthrogram obtained with application of leg traction shows massive hypertrophy of labrum with diffuse contrast interposition, consistent with retear (arrowheads) and unstable chondrolabral flap (arrow). Anchor from labrum refixation (asterisk) is evident.