

Abstract
Rosacea is a chronic, often progressive disorder characterized by facial erythema, telangiectasias, papules, pustules, and/or rhinophyma. In this study, we investigated the tissue structure in rosacea compared to controls. We performed a case–control study between five patients with mild‐to‐moderate erythematotelangiectatic rosacea (ETR) and five matched controls. Facial biopsy samples from rosacea patients and controls were stained with picrosirius red for collagen and CD31 for microvessel identification. Mean collagen content was significantly greater in control samples (19.603% ±8.821%) compared to rosacea samples (16.812% ± 7.787%, p = 0.030). In contrast, mean microvessel density was significantly higher in rosacea patients (4.775 E‐5 ± 1.493 E‐5 µm−3) compared to controls (2.559 E‐5 ± 8.732 E‐6 µm−3, p = 0.004). Mean microvessel lumen area was also significantly higher in rosacea patients (491.710 ± 610.188 µm2) compared to controls (347.879 ± 539.624 µm2, p = 0.003). We identified a correlation between decreased collagen content and increased microvessel size and density in rosacea patients that was not observed in controls. These structural changes to the dermal matrix may contribute to the characteristic vessel growth and dilation in rosacea.
Keywords: collagen, photoaging, rosacea, telangiectasia, telangiectatic photoaging
While control samples displayed significantly greater mean collagen content compared to rosacea samples, mean microvessel density as well as mean microvessel lumen area were significantly higher in rosacea patients than in controls.

1. INTRODUCTION
Rosacea affects over 16 million Americans, and individuals with rosacea may suffer serious psychosocial ramifications from this condition. The precise pathogenesis of rosacea has yet to be fully elucidated. Factors promoting rosacea include abnormalities in innate immunity, vascular hyperreactivity, gastrointestinal disorders, genetic predisposition, and ultraviolet (UV) exposure (Powell, 2000; Powell, 2005; Wilkin, 1994; Wilkin, et al, 2002; Wilkin, et al, 2004).
In fact, erythema and telangiectasias, categorized as erythematotelangiectatic rosacea (ETR), tend to appear more prominently in skin regions prone to atrophic photoaging as a result of UV exposure. Some of the mechanisms of UV‐induced photoaging may also be involved in the pathophysiology of rosacea (Steinhoff, et al, 2013). UV irradiation promotes photoaging by inducing collagen‐degrading matrix metalloproteinases (MMPs) and by suppressing collagen production (Fisher, et al, 2008). The impact of MMP‐1‐mediated collagen degeneration on endothelial cells has been shown to lead to the formation of vascular tubes. These vascular tubes resemble the lumen of telangiectasias (Varani, et al, 2008). Similarly, we suspect that photoaging‐induced damage to the dermal matrix may have a role in inducing the increased vascularity and telangiectasias observed in ETR.
2. METHODS
We performed a case–control study between rosacea patients and matched controls to examine the associations between the clinical features of rosacea, collagen degeneration, and microvascular changes. Our study included five patients with mild‐to‐moderate ETR ages 47‐83 and five controls matched by age ±2 years and race. The study was approved by the Johns Hopkins Institutional Review Board. Written informed consent was obtained from all participants. Each participant underwent clinical evaluation to determine severity of rosacea and/or photoaging using the National Rosacea Society clinical grading system and the Griffiths photonumeric photodamage scale (Griffiths, et al, 1992; Wilkin, et al, 2004). Three‐mm punch biopsies were taken of telangiectasias from rosacea patients and of normal facial skin from their matched controls. The control samples consisted of facial skin biopsies of healthy volunteers enrolled in our study. Biopsy samples were stained with Picrosirius red for collagen visualization (Figure 1) and CD31 for blood vessels (Figure 2). The Image J color thresholding tool was used to quantify collagen content (%) per random section as previously described (Bauman, et al, 2014). In this study, collagen content was used as a surrogate marker for intact collagen. Image J was also used to compute microvessel density and mean microvessel lumen area of each CD31‐stained slide. Five random sections were used for this analysis. In each random section, microvessel density was calculated by manually counting the number of microvessels within the slide. The microvessel number was then divided by Image J‐calculated area (in μm2) of each sample on the slide. The lumen area of every microvessel in each random section was computed with the Image J vessel area tool. The mean microvessel lumen area was then calculated for each sample. Paired sample t‐tests in SPSS‐25 were used to compare collagen content and microvessel characteristics between rosacea patients and their matched controls. The microvessel lumen areas calculated within each sample were furthermore compared within each of the five individual patient–control pairs using independent sample t‐tests in SPSS‐25 (Table 1).
FIGURE 1.
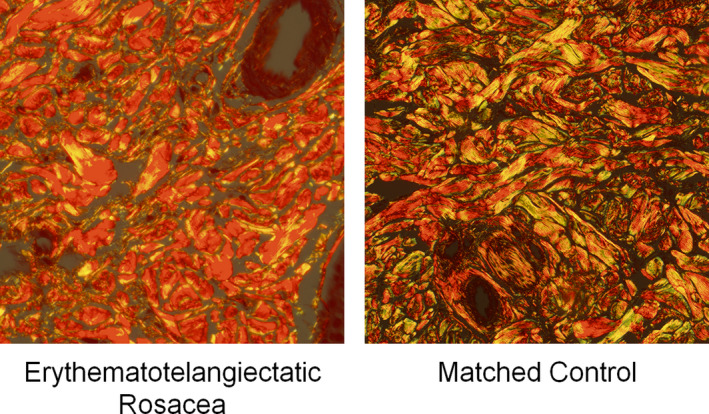
Picrosirius red‐stained facial biopsy samples at 40× magnification from a telangiectasia in a patient with erythematotelangiectatic rosacea (ETR) and from normal skin in the matched control. Mean collagen content was significantly diminished in patients with ETR (16.812% ± 7.787%) compared to controls (19.603% ± 8.821%, p = 0.030)
FIGURE 2.
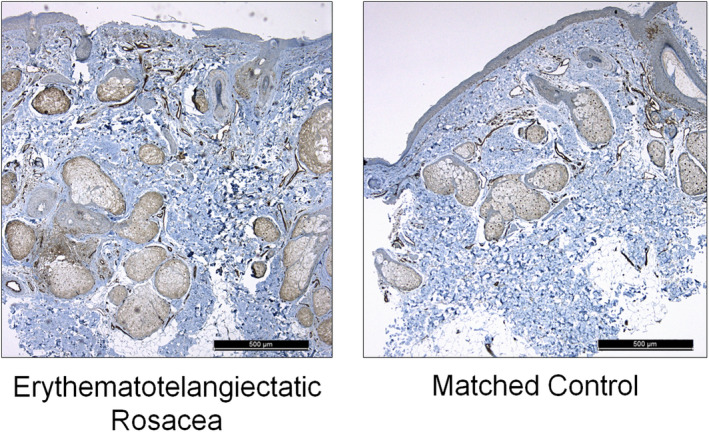
CD31‐stained facial biopsy samples at 5x magnification from a telangiectasia in a patient with erythematotelangiectatic rosacea (ETR) and from normal skin in the matched control. Mean microvessel lumen area and microvessel density were significantly higher in patients with ETR (density 4.775 E‐5 ± 1.493 E‐5 µm−3, lumen area 491.710 ± 610.188 µm2) compared to controls (density 2.559 E‐5 ± 8.732 E‐6 µm−3, p = 0.004; lumen area 347.879 ± 539.624 µm2, p = 0.003)
TABLE 1.
Summary of mean collagen content, microvessel lumen area, and microvessel density between rosacea patients (n = 5) and matched controls (n = 5)
| Rosacea | Control | p value | |
|---|---|---|---|
| Mean Collagen Content (%) ±SD | 16.812 ± 7.787 | 19.603 ± 8.821 | 0.030 |
| Mean Microvessel Lumen Area (µm2) ±SD | 491.710 ± 610.188 | 347.879 ± 539.624 | 0.003 |
| Mean Microvessel Density (µm−3) ±SD | 4.775 E‐5 ± 1.493 E‐5 | 2.559 E‐5 ± 8.732E‐6 | 0.004 |
3. RESULTS AND DISCUSSION
A summary of participant demographics, clinical grading, and histologic findings by individual biopsy sample is located in Table S1. When examining the dermis of Picrosirius red‐stained slides, control samples displayed significantly greater mean collagen content (19.603% ±8.821%) compared to rosacea samples (16.812% ±7.787%, p = 0.030). The mean microvessel density in rosacea patients (4.775 E‐5 ± 1.493 E‐5 µm−3) was significantly higher than in controls (2.559 E‐5 ± 8.732 E‐6 µm−3, p = 0.004). Likewise, the mean microvessel lumen area in rosacea (491.710 ± 610.188 µm2) was significantly higher than in controls (347.879 ± 539.624 µm2, p = 0.003). By individual patient–control pair, all five rosacea patients had increased microvessel density and decreased collagen content compared to their individually matched control. In 3/5 patient–control pairs, mean microvessel lumen area was increased to a statistically significant degree in rosacea patients compared to their matched controls. No significant correlations were identified between these microscopic findings and the clinical severity of rosacea or photoaging.
Our findings were consistent with a recent study evaluating the histologic and molecular differences between ETR and telangiectatic photoaging (TP), which demonstrated increased vessel dilation in facial biopsies of patients with ETR compared to controls (Helfrich, et al, 2015). While MMP‐1, −3, and −9 expression was significantly elevated between ETR and controls, MMP‐3 expression was also significantly elevated between patients with ETR and TP (Helfrich, et al, 2015). Our study furthermore demonstrated a correlation between decreased collagen content and increased microvessel size and density in rosacea patients that was not observed in controls. These structural changes to the dermal matrix may represent early aberrations involved in promoting the progression of rosacea. Our study was limited by a small sample size. Future studies with larger sample sizes would be useful in further elucidating the relationship between photodamage and rosacea.
ETHICAL STANDARDS
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Johns Hopkins institutional review board and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from all individual participants included in the study.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to disclose.
AUTHOR CONTRIBUTIONS
KT contributed to the data analysis/interpretation, drafting the manuscript, and critical revision of the manuscript. BM, SL, and JQ contributed to the concept/design of the study and acquisition of data. SK and AC contributed to all aspects of the study. All authors have read and approved the final manuscript.
Supporting information
Table S1
REFERENCES
- Bauman, T.M. , Nicholson, T.M. , Abler, L.L. , Eliceiri, K.W. , Huang, W. , Vezina, C.M. et al. (2014) Characterization of fibrillar collagens and extracellular matrix of glandular benign prostatic hyperplasia nodules. PLoS One, 9(10), e109102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fisher, G.J. , Varani, J. & Voorhees, J.J. (2008) Looking older: fibroblast collapse and therapeutic implications. Archives of Dermatology, 144(5), 666–672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffiths, C.E. , Wang, T.S. , Hamilton, T.A. , Voorhees, J.J. & Ellis, C.N. (1992) A photonumeric scale for the assessment of cutaneous photodamage. Archives of Dermatology, 128(3), 347–351. [PubMed] [Google Scholar]
- Helfrich, Y.R. , Maier, L.E. , Cui, Y. , Fisher, G.J. , Chubb, H. , Fligiel, S. et al. (2015) Clinical, histologic, and molecular analysis of differences between erythematotelangiectatic rosacea and telangiectatic photoaging. JAMA Dermatology, 151(8), 825–836. [DOI] [PubMed] [Google Scholar]
- Powell, F.C. (2000) What’s going on in rosacea? JEADV., 14, 351–352. [DOI] [PubMed] [Google Scholar]
- Powell, F.C. (2005) Clinical practice: Rosacea. New England Journal of Medicine, 352(8), 793–880. [DOI] [PubMed] [Google Scholar]
- Steinhoff, M. , Schauber, J. & Leyden, J.J. (2013) New insights into rosacea pathophysiology: a review of recent findings. Journal of the American Academy of Dermatology, 69, S15–26. [DOI] [PubMed] [Google Scholar]
- Varani, J. , Perone, P. , Warner, R.L. , Dame, M.K. , Kang, S. , Fisher, G.J. et al. (2008) Vascular tube formation on matrix metalloproteinase‐1‐damaged collagen. British Journal of Cancer, 98(10), 1646–1652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilkin, J.K. (1994) Rosacea: pathophysiology and treatment. Archives of Dermatology, 130, 359–362. [DOI] [PubMed] [Google Scholar]
- Wilkin, J. , Dahl, M. , Detmar, M. , Drake, L. , Feinstein, A. , Odom, R. et al. (2002) Standard classification of rosacea: Report of the national rosacea society expert committee on the classification and staging of rosacea. Journal of the American Academy of Dermatology, 46(4), 584–587. [DOI] [PubMed] [Google Scholar]
- Wilkin, J. , Dahl, M. , Detmar, M. , Drake, L. , Liang, M.H. , Odom, R. et al. (2004) Standard grading system for rosacea: Report of the national rosacea society expert committee on the classification and staging of rosacea. Journal of the American Academy of Dermatology, 50(6), 907–912. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1