
Figure 1:
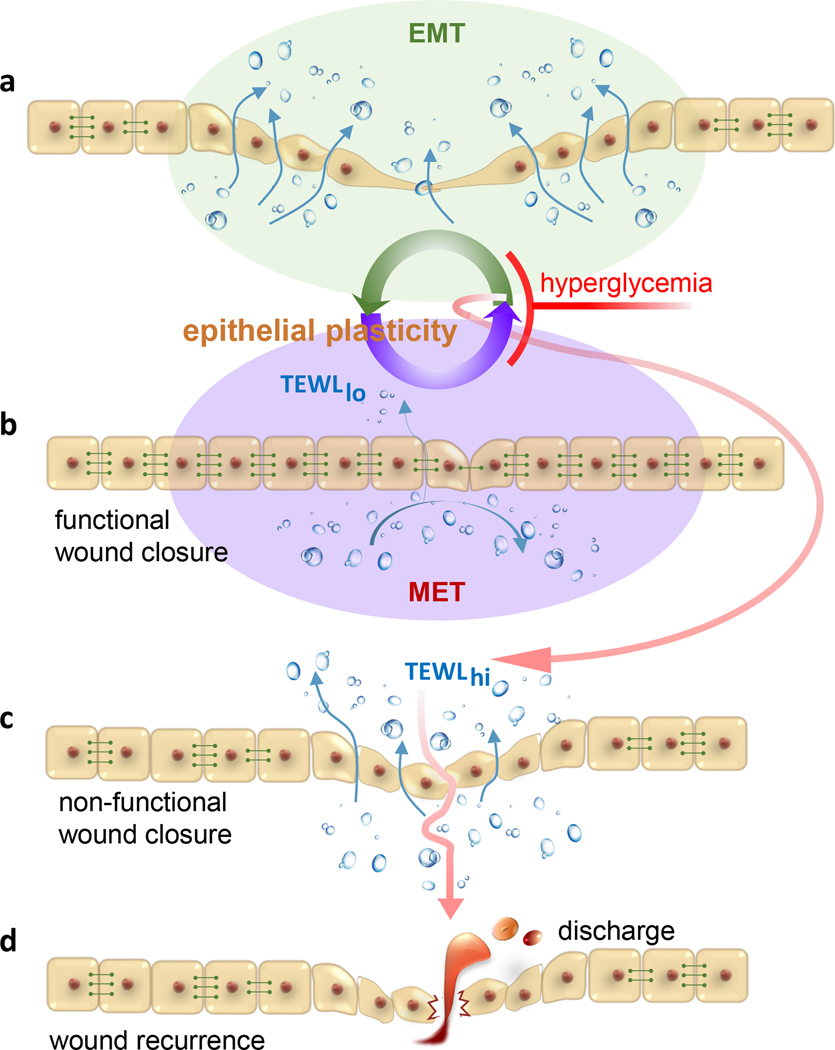
Hyperglycemia restrains cutaneous epithelial plasticity necessary for functional wound closure. A hypothetical paradigm depicts a-b wherein EMT↔MET is central for re-epithelialization and restoration of barrier function of the repaired skin. During EMT, epithelial cells dismantle cell adhesion and tight junction structures in an effort to acquire a mesenchymal phenotype favoring re-epithelialization. MET helps reconstitute apical junctional complexes (AJC) restoring barrier function of the repaired skin. Hyperglycemia is a barrier to such plasticity and as such hinders re-epithelialization, restoration of barrier function or both (c). The result is wound chronicity or non-functional wound closure. Closure of wound without restoration of skin barrier function predisposes the closed wound to recidivism (d) as evident in preclinical porcine studies. The incidence of wound recurrence is high in diabetic patients. TEWL, transepidermal water loss is a measure of skin barrier function. TEWLhi, deficient skin barrier function; TEWLlo, restored skin barrier function indicative of functional wound closure. Horizontal rivets between cells represent functional AJC. These are low or absent in mesenchymal cells compromising barrier function.