
Fig. 1.
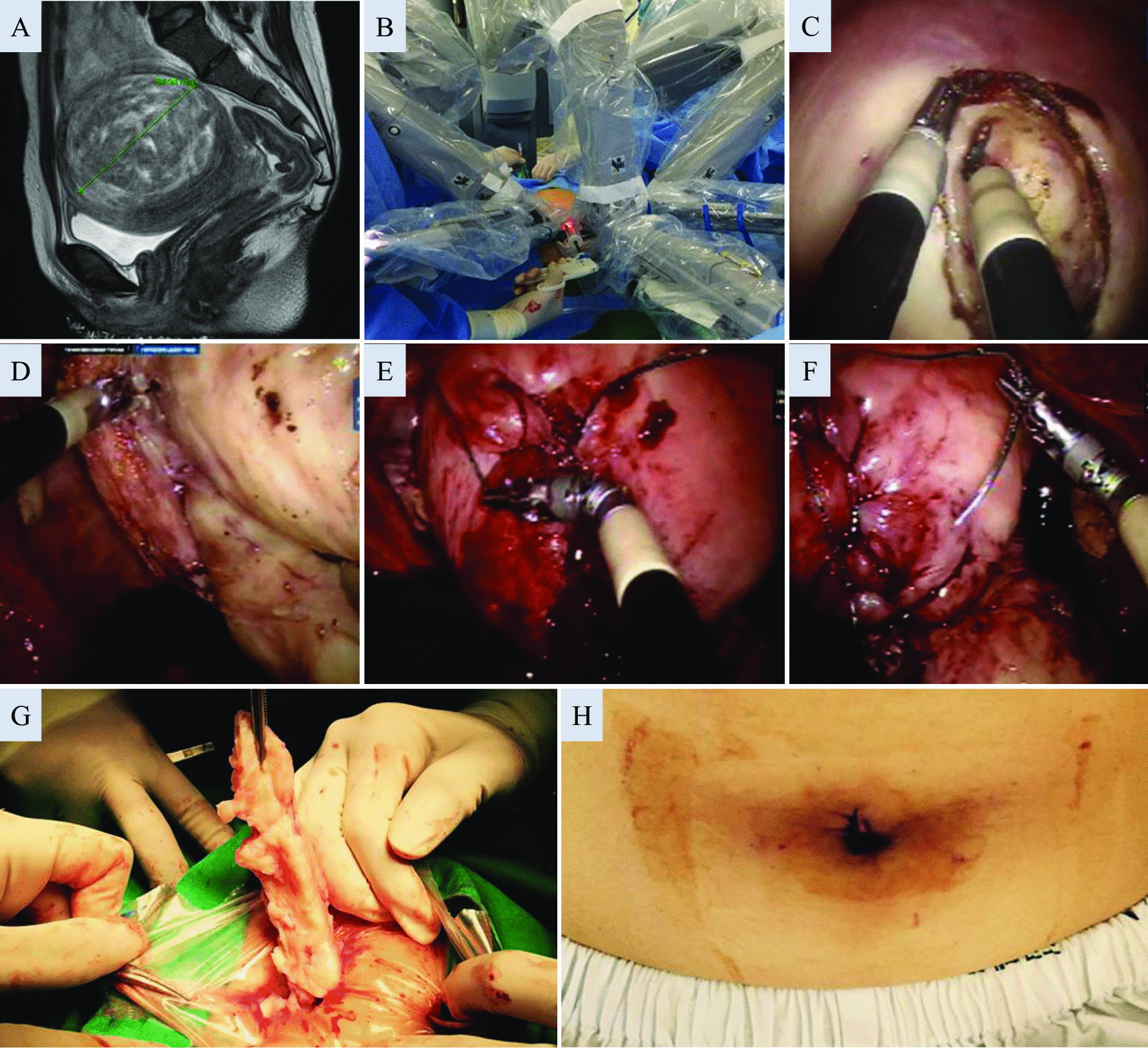
A stepwise description of a representative robotic single-site myomectomy case. Myomectomy was recommended for a 32 year-old woman due to menorrhagia and infertility for a period of 14 months. To decrease the size of this 8.5-cm FIGO type 3 myoma, leuprolide acetate was injected, but surgery could not be postponed due to intolerable heavy vaginal bleeding for 3 weeks. A Due to the unusual amount of bleeding and suspected distortion of the uterine cavity on ultrasonography, a pelvic magnetic resonance imaging was performed prior to the surgery (T2-weighted image). B A view of the operating field after docking of the Da Vinci Si single-site platform, with the first assistant to the right of the patient controlling the assistant port. The maintenance of this configuration of the robotic arms is important to create adequate triangulation intra-abdominally and to minimize tool clashing. C The myometrial incision was placed with a monopolar hook. D Although the robotic tools for the single-site platform have less variety, skillful use of bipolar forceps, the hook, and/or the wristed needle driver allows for adequate dissection. E Suturing was performed with V-locks in three layers, involving deep myometrial sutures to achieve adequate approximation and to prevent dead spaces from forming within the myometrium. F Although the serosal layer is most commonly approximated with Vicryls, when barbed suture materials are used, continuous sutures are placed so that the barbing is not exposed, and an anti-adhesive film is covered at the end. G Manual in-bag morcellation of the myoma with spiral incisions through the 2.5-cm umbilical port. H The 2.5-cm umbilical incision immediately after closure