
Figure 1. The asymptomatic and symptomatic phases of DCM.
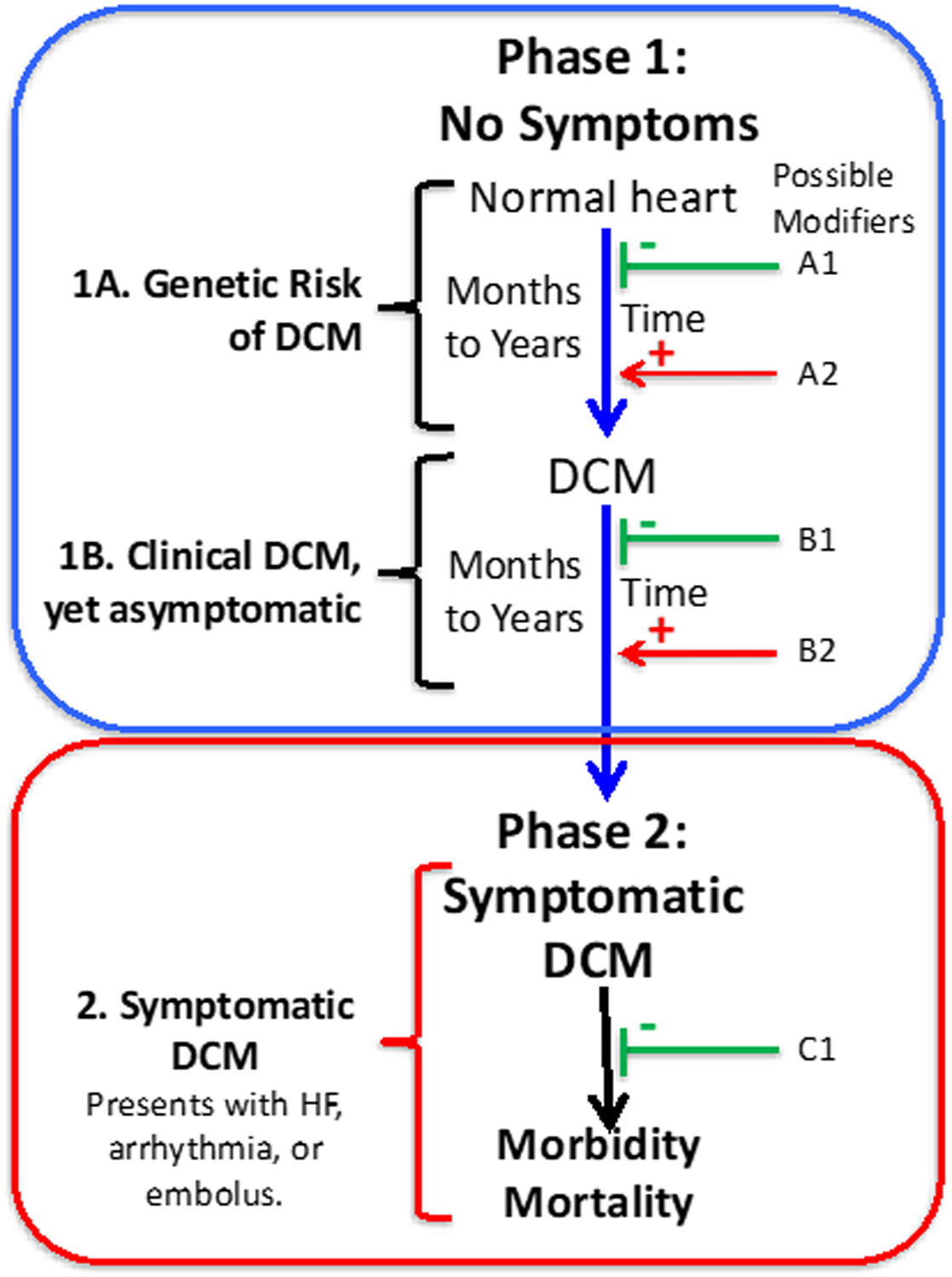
The causal pathway of DCM is illustrated, as adapted,16, 30 in adult-onset DCM. Phase 1 includes two periods, both asymptomatic. In the first period (1A), individuals who harbor rare DCM variants have risk of developing DCM over time. Genetic information identifies the individuals who would benefit from periodic clinical screening to detect early clinical disease. In Phase 1B, DCM can be clinically detected by appropriate imaging studies but remains asymptomatic, evading detection for years unless surveillance clinical screening is undertaken to detect it. In Phase 2, the individual with DCM develops symptoms, most commonly with HF, which triggers a medical evaluation with a diagnosis of HF and the eventual discovery of the underlying DCM. Factors that may diminish or block these causal pathways to DCM or HF are shown in green (A1, B1, C1)); environmental factors could include good nutrition, a low salt diet, low blood pressure, or drug therapy (e.g., angiotensin-converting enzyme inhibitors or β-blockers). Factors that may accelerate the causal pathway to DCM or HF are shown in red (A2, B2); examples include hypertension, alcohol use, or exposure to chemotherapy or other myocardial toxins. Genomic modifiers, both injurious or protective, include rare, low frequency or common variants that could be operative at all points. Detection of a “pre-DCM phenotype” that portends the transition from Phase 1A to Phase 1B could permit earlier introduction of conventional medical therapy in an effort to block the development of DCM. Following the transition to Phase 1B, all efforts need to be made to prolong this phase to avert late phase symptomatic disease in Phase 2.