
Fig 1. Mapping of alternative therapies for DED based on present underlying pathologies.
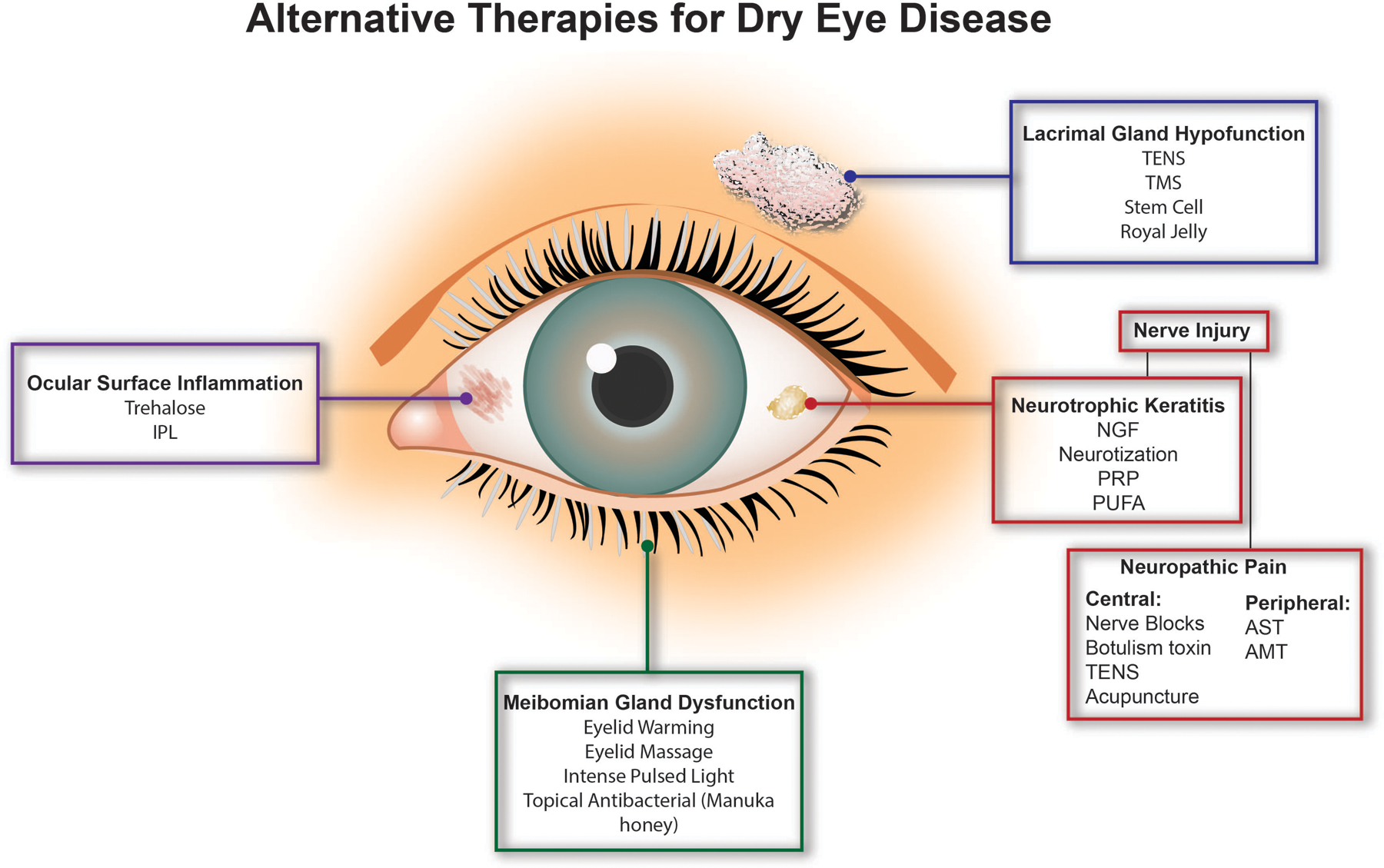
Alternative and adjunct therapies have been developed to treat various underlying causes of DED. Patients with aqueous deficient DED due to lacrimal gland hypofunction may benefit from transcutaneous electrical nerve stimulation (TENS), transcranial magnetic stimulation (TMS), stem cell therapy, or royal jelly therapy. Alternatively, those with evaporative DED due to meibomian gland dysfunction may be treated with office-based eyelid warming and massage devices, intense pulsed light therapy, and topical antibacterial agents, such as Manuka honey. Several therapies are currently available to target DED associated ocular surface inflammation. Trehalose and intense pulsed light therapy are two adjuvant therapies that are also being studied for this purpose. Lastly, nerve dysfunction may also be present in DED. Treatments for neurotrophic keratitis include nerve growth factor (NGF), platelet rich products (PRP), corneal neurotization, and polyunsaturated fatty acids (PUFA). In patients with neuropathic pain, cutaneous nerve blocks, TENS, botulinum toxin, and acupuncture have been used to treat pain of central origin, while autologous serum tears (AST) and amniotic membrane transplant (AMT) have been used to treat pain of peripheral origin.