
Figure 4. Contractile function and calcium transients from isolated cardiomyocytes in sham, sham+empagliflozin, transverse aortic constriction and transverse aortic constriction +empagliflozin groups.
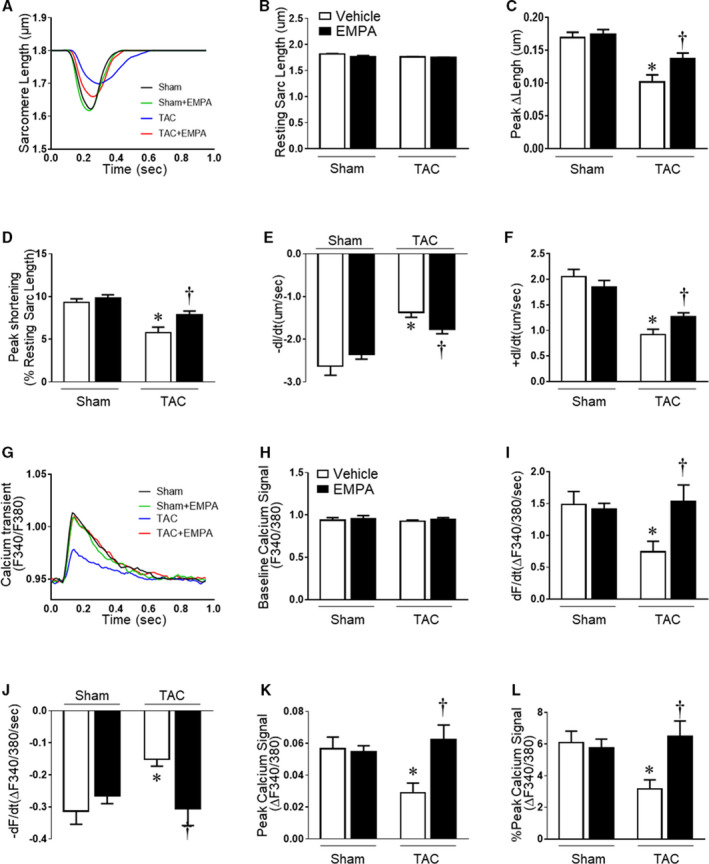
(A) Representative traces of cell contraction by time using 1Hz. (B) Resting sarcomere length; (C) Maximum cardiomyocyte contraction (Peak ∆length). (D) Shortening length normalized by resting sarcomere length (Peak shortening); (E) Maximum contraction velocity (−dL/dt); (F) Maximum relaxation velocity (+dL/dt); (G) Representative fluorescent traces of F340/380 ratios of cardiomyocytes loaded with Fura 2‐AM calcium transient using 1 Hz stimulation; (H) Baseline calcium signal (F340/380); (I) Maximum calcium change velocity during contraction (+dF/dt); (J) Maximum calcium change rate during relaxation(−dF/dt). (K) Maximum calcium amplitude transient (Peak calcium signal); (L) Maximum calcium transient amplitude normalized by baseline calcium signal (% Peak calcium signal). Results are expressed as mean±SEM, n=5–6 mice per group (40–92 cells were measured for each animal). One‐way ANOVA (non‐repeated measures) (B–F and H–L). TAC indicates transverse aortic constriction. *P<0.05 vs sham, † P<0.05 vs transverse aortic constriction.