
fig 2.
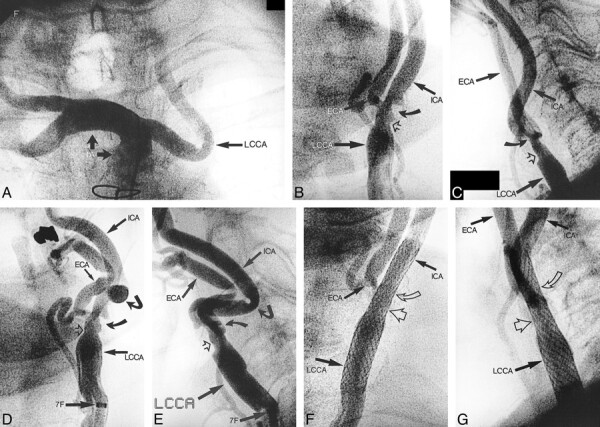
Angiograms from the case of an 87-year-old female patient with occlusion of the right internal carotid artery and 65% symptomatic, ulcerated stenosis on the left common and internal carotid arteries.
A, Angiogram of the innominate artery (IA) shows a 90-degree take-off of the left common carotid artery (LCCA), with more distal tortuosity.
B, Anteroposterior projection angiogram of the left common carotid artery (LCCA) (5F catheter in the ostium). Sixty-five percent ulcerated stenosis (curved arrow) on the internal carotid artery (ICA) and on the common carotid artery (open arrow) can be seen. ECA, external carotid artery.
C, Lateral projection.
D, Anteroposterior projection angiogram of the left common carotid artery (LCCA), obtained through a 7F sheath placed in the distal left common carotid artery. By upward displacement of the bifurcation, kink (angled arrow) developed in the proximal internal carotid artery. 7F, distal tip of the 7F sheath; ECA, external carotid artery; open arrow, stenosis in the distal left common carotid artery; curved arrow, ulcerated stenosis in the internal carotid artery.
E, Lateral projection.
F, Anteroposterior projection angiogram of the left common carotid artery (LCCA), obtained after CAS was performed. A 10 × 20 Wallstent was used, dilated with a 5.5 × 20 Symmetry balloon. The 7F sheath is removed; the 5F catheter is in the ostium of the left common carotid artery. Open curved arrow, previous location of the ulcerated stenosis on the internal carotid artery.
G, Lateral projection.