
fig 2.
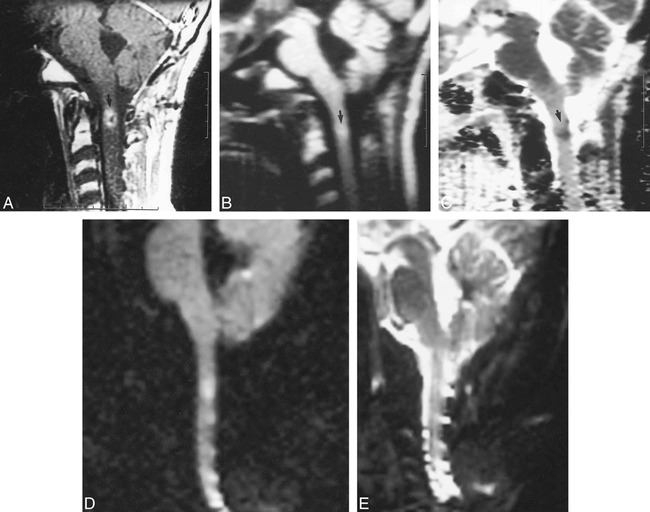
Case of a 16-year-old male patient with medulloblastoma treated with craniospinal radiation with presumed radiation effect at the site of overlap of the cranial and spinal radiation fields in the upper cervical spinal cord. Based on the intramedullary location of the lesion, metastatic medulloblastoma was considered unlikely. On follow-up images several months later (not shown) the lesion resolved. No anti-cancer therapy was undertaken during that time, and radiation effect was therefore considered to have been the most likely cause of the lesion.
A, Sagittal contrast-enhanced T1-weighted image (600/20/2) of the cervical spine shows intramedullary enhancement (arrow).
B, Sagittal LSDI isotropic high b factor diffusion image (2014/95/1, 4-mm section thickness, b = 750 s/mm2 extrapolated to 1000 s/mm2, six directions) shows increased signal within the lesion (arrow).
C, Sagittal LSDI trace ADC map shows low intensity within the lesion confirming decreased diffusion (arrow).
D, Sagittal EPDI isotropic high b factor diffusion image (4999/108/1, 5-mm section thickness, b =1000 s/mm2, three directions) shows artifactual high signal intensity in multiple locations in the cervical spinal cord.
E, Sagittal EPDI trace ADC map is degraded by artifact and does not show the lesion seen on both the conventional MR and the LSDI sequences.