
fig 5.
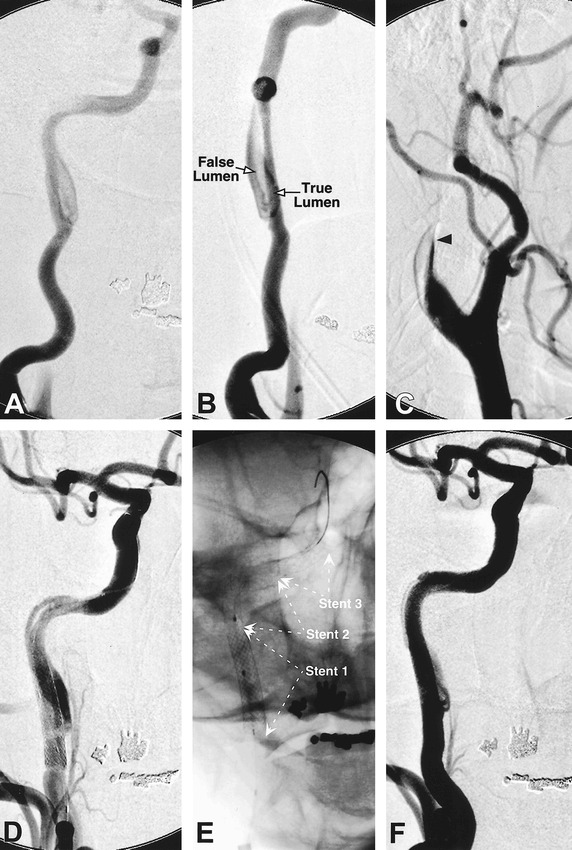
A 51-year-old man (patient 3) developed sudden loss of vision in the left eye, a left Horner's syndrome, and orthostatic lightheadedness. Digital subtraction angiography with injection of the right common carotid artery shows intimal dissection of the right internal carotid artery in the high cervical region, with delineation of the true and false lumen (A, B). Injection of the left common carotid artery, which had evidence of dissection but was shown to be patent on an angiogram obtained 4 days earlier, now reveals complete left internal carotid artery occlusion (arrowhead) despite systemic anticoagulation (C). A Rapid Transit microcatheter was used to catheterize the true lumen, followed by deployment of a Wallstent (6 mm × 20 mm) in the proximal portion of the dissected segment (D). Persistent filling of the false lumen, however, required the tandem placement of two additional GFX stents (4 mm × 12 mm) in the petrous segment of the right internal carotid artery (E), with reconstitution of the normal luminal diameter (F)