
Figure 2.
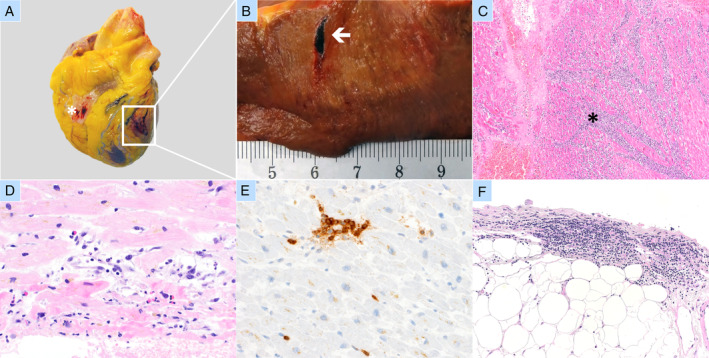
Independently occurring concurrent active lymphohistiocytic perimyocarditis and acute myocardial infarction with transmural perforation in a case of lethal COVID‐19. (A–C) Acute myocardial infarction. (A) Gross findings – haemorrhagic diathesis of epicardium (*); transmural perforation of the anterior myocardial wall (white box). (B) Close‐up view of perforation (white arrow) with gross signs of acute infarction (territorial parenchymal pallor and yellowish discolouration). (C) Acute myocardial infarction in the region of perforation with territorial coagulation necrosis and dense infiltrates of neutrophilic granulocytes (black asterisk). (D–F) Active lymphohistiocytic myocarditis. (D) Lymphohistiocytic infiltrates and few eosinophils associated with necrotic hypereosinophilic cardiomyocytes with contraction bands; (E) cluster of T‐lymphocytes (CD3 IHC, ×400); (F) lymphocytic infiltrate in the epicardial fat.