
Figure 1.
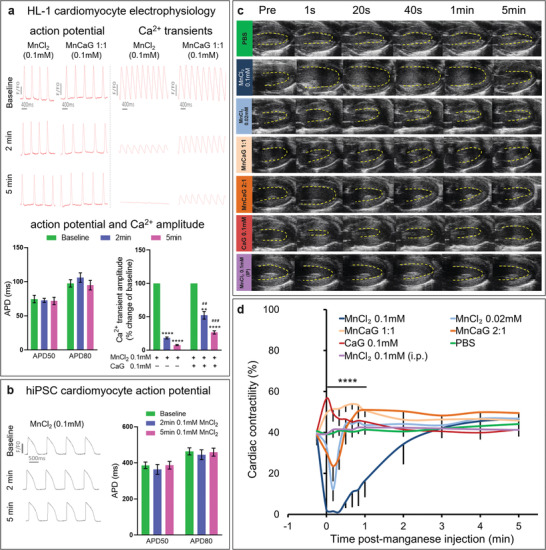
Effects of manganese on cardiac electrophysiology and function: a) Upper panel: Representative optical action potential and Ca2+ transient traces from HL‐1 cardiomyocytes at baseline and at 2 and 5 min after superfusion with 0.1 mM MnCl2 with/out CaG supplement. Lower panel: APD50 and APD80 were not affected by 0.1 mM MnCl2 (n = 5), but Ca2+ transient amplitude was reduced by 0.1 mM MnCl2 and partially restored by supplement with 0.1 mM CaG (n = 4). Data were analyzed by paired two‐tailed Student's t‐test to compare with baseline **p = 0.0011 ****p < 0.0001 and unpaired two‐tailed Student's t‐test to compare MnCl2 to MnCl2+CaG‐ ## p = 0.0011 ### p = 0.0003). b) Representative optical action potential traces from human iPSC derived cardiomyocytes at baseline and at 2 and 5 min after superfusion with 0.1 mM MnCl2. APD50 and APD80 were not affected by 0.1 mM MnCl2 (n = 6). c) Representative end systolic ultrasound images acquired before and after injection of the compounds indicated. d) Time course of myocardial contractility quantified as fractional shortening showed immediate reduction in myocardial contractility after i.v. infusion of 0.1 mM MnCl2 (n = 6) which can be reversed when Mn2+ was supplemented with CaG (MnCaG) at either 1:1 or 2:1 MnCl2 to CaG ratio (n = 6). Mean value ± standard error mean (SEM). Data were compared between groups at each time point by one‐way ANOVA (****p < 0.0001 at 1 s to 1 min post injection) and compared to baseline in each group using two‐way repeated measures ANOVA followed by Dunnett's post hoc test (Table S1, Supporting Information). Raw data are presented in Table S1 in the Supporting Information.