

Abstract
Even though cardiovascular disease (CVD) kills more women than men each year and remains a leading cause of death in women, it is a common misconception that women are less likely to develop CVD. Considerable sex difference exists between men and women with regard to prevention, investigations, and management of CVD. Coronary artery disease (CAD) is a major contributor to CVD morbidity and mortality and hence is specifically addressed in this article. With an explosive increase in the incidence of conventional risk factors for coronary artery disease in India, there has been an alarming increase in women's coronary events as much as men. A false sense of gender-based protection by estrogen leads to less aggressive and late prevention or management strategies that contribute to women's CAD. Metabolic syndrome (MetS) is an important contributor to future development of CAD and is also an indicator for earlier interventions for prevention. Due to physical inactivity and central obesity, MetS is more prevalent in women, especially postmenopausal. With estrogen loss, menopause marks a critical cardiovascular biological transition, with a significantly increased CVD risk in women aged >55 years. Certain female-specific risk factors, such as history of polycystic ovarian syndrome, pregnancy-induced hypertension, and gestational diabetes, also seem to play an essential role in the development of CVD in later life. Certain vascular and biological factors, such as smaller coronary vessel size, higher prevalence of small vessel disease, and lesser development of collateral flow, also play an important role. This review article is an attempt to provide important information on gender differences in CVD with specific emphasis on CAD.
KEYWORDS: Cardiovascular disease, coronary artery disease, estrogen, gender differences, menopause, prevention, risk factors, women
INTRODUCTION
It is common knowledge that estrogen-like hormones protect women in premenopausal years, and it is observed that generally, the cardiovascular disease (CVD) develops 8–10 years later in women than in men. However, women quickly catch up with men after menopause, and CVD is still the major cause of death in women over 55 years.
Menopause marks an important cardiovascular biological transition, with a significantly increased CVD risk in women aged >55 years. Estrogen loss seems to have negative effects on arterial function and adversely alters the cholesterol profile, increases blood pressure, and increases the prevalence of metabolic syndrome (MetS) and truncal obesity.
With the alarmingly increasing incidence of conventional risk factors such as physical inactivity, diabetes, hypertension, stress, and dyslipidemia, there has been a significant increase in the prevalence of myocardial infarction in midlife (35–54 years of age) women. There has been a fourfold rise of CAD prevalence in India during the past 40 years. Current estimates from epidemiological studies from various parts of the country indicate a prevalence of CAD to be between 7% and 13% in urban[1,2,3] and 2% and 7% in rural[4,5] populations. Higher incidence in Indians was attributed, to a large extent, to genetic factors and South Asian ethnicity. However, the famous INTERHEART study established that more than 90% of risk of first myocardial infarctions was attributable to easily measurable and modifiable known risk factors such as physical inactivity, obesity, diabetes, hypertension, tobacco, psychological stress, high cholesterol, and insufficient fruit and vegetables intake.[6]
In a study done in North Indians, the prevalence of MetS was found to be crossing 40% with higher incidence in women than men.[7] Indian women having MetS were also found to be having higher prevalence of high triglycerides, hyperglycemia, and obesity, than men, increasing their risk of CAD further.
METABOLIC SYNDROME
MetS is a cluster of conditions that include high blood pressure, high blood sugar, excess body fat around the waist, and abnormal lipid levels (low high-density lipoproteins [HDL] and high triglycerides). These significantly increase the risk of CVD and diabetes. Menopausal transition brings about a change in total body composition characterized by an increased body fat mass and central adiposity. This creates a compatible atmosphere for abnormal metabolism and aggravated cardiometabolic risk factors.[7,8] The changing hormonal status with altered estrogen levels is an important cause of metabolic syndrome at menopausal transition. In a study done by Government Medical College, Amritsar, Punjab,[9] the incidence of MetS was found to be higher in postmenopausal women (42%) than in premenopausal women (16%), clearly emphasizing the need of lifestyle modification to reduce the emergence of MetS and CVDs. Reduced levels of estrogen have been associated with metabolic alterations and increased insulin resistance (IR) in postmenopausal women, and IR may predispose women to increased CVD risk.[10]
Abnormal waist circumference was found to be the most prevalent and responsible component for MetS and also for insulin resistance.[11,12] In a study done in Northern Indians, prevalence of metabolic syndrome was found to be crossing 40% with higher incidence in women than men.[13] Indian women having metabolic syndrome were also found to be having higher prevalence of high triglycerides, hyperglycemia and obesity, compared to men, increasing their risk of CAD further.
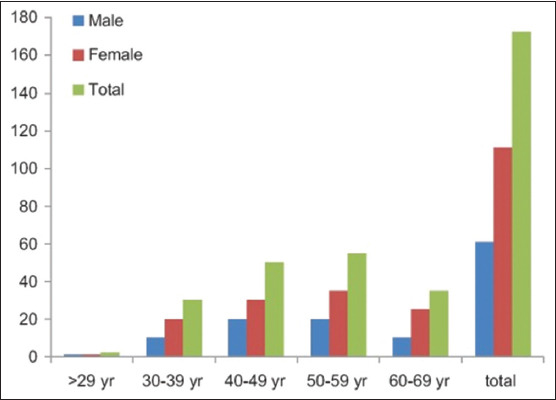
Age and sex distribution of 172 metabolic syndrome cases is presented in Table 1. Nearly 80% of the MetS patients were >40 years of age and the prevalence was significantly high in females.[13]
Table 1.
Age and sex distribution of 172 cases ofmetabolic syndrome
The medical research in the past decade has identified a spectrum of risk factors for cardiovascular diseases that may be specific to women. These female-specific risk factors, which may include early menopause, hypertensive disease of pregnancy, gestational diabetes, polycystic ovarian syndrome (PCOS), and depression, confer significant additional risk in women besides the traditional risk factors. Gender-based variations in presenting symptoms; electrocardiograms (ECG)/treadmill test (TMT) interpretations and even coronary angiographic ndings (absence of major epicardial artery disease in some women even in presence of typical ischemic symptoms and ECG/echocardiogram (ECHO) ndings).[14,15,16]
Gender differences of various vascular and biological factors, such as loss of protective estrogen effects on vasculature, smaller coronary vessel size, lower coronary flow reserve, higher prevalence of small vessel disease, and lesser development of collateral flow, also play an essential role. At younger age, women more often have acute coronary syndromes (ACS) with angiographically “normal” coronary arteries than men.[14,15,16]
Relatively lower self-awareness among women; and a lower index of suspicion on the part of treating doctors, all of these result in misdiagnosis or delayed diagnosis, less aggressive treatment, and lower outcomes.
EPIDEMIOLOGY, ROLE OF ESTROGENS, AND MENOPAUSE
Estrogen is thought to act through estrogen receptors expressed both in vascular endothelial and smooth muscle cells. It improves the arterial wall response to injury, promotes re-endothelialization, and inhibits smooth muscle cell proliferation and matrix deposition following vascular injury. Estrogen also prevents coronary artery spasm through vasodilatation mediated by both rapid increases in the production of nitric oxide (NO) and the induction of NO genes.
During the premenopausal years, endogenous estrogens protect against the atherosclerotic disease in women. Before menopause, the CHD event rate in women is low and predominantly attributed to clustering of conventional CAD risk factors and/or estrogen deficiency. In the Women's Ischemia Syndrome Evaluation (WISE) study, it was shown that young women with endogenous estrogen deficiency have a more than sevenfold increase in CAD risk. Estrogens effect several metabolic factors, such as lipids, inflammatory markers, and the coagulant system. They also promote a direct vasodilatory effect through the α- and β-receptors in the vessel wall. Furthermore, signs of subclinical atherosclerosis, as visualized by intima–media thickness measurements, can already be found in women before menopause, especially when several CHD risk factors are present.
Female-specific risk factors
-
PCOS and metabolic syndrome:
PCOS is associated with an unfavorable cardiometabolic profile in early life. Apart from dyslipidemia, other causes such as obesity, onset of type 2 diabetes, and androgens are thought to influence cardiovascular health.[12,17]
Flow-mediated dilatation (FMD) is a technique developed to measure vascular dysfunction.
Glintborg et al. concluded that the event rate of CVD including hypertension and dyslipidemia is higher in PCOS compared to control.
Women with gestational diabetes mellitus (GDM): Normally abnormal glucose levels subside in 4 to 6 weeks in GDM after delivery however in about 10-20 % of cases abnormal glucose tolerance persist. They may develop type 2 diabetes mellitus. This adds to increase risk of CVD and requires special measurement to detect and manage properly.[18]
-
Women with hypertensive history during pregnancy and placental syndrome which often leads to poor fetal growth or intrauterine death (IUD):
There is a higher risk of vascular disturbances in these groups of patients with persistent hypertension after delivery and even later stage of life.[19,20]
GENDER DIFFERENCES IN CONVENTIONAL CORONARY ARTERY DISEASE RISK FACTORS
Although well-recognized conventional CAD risk factors (such as diabetes, hypertension, cholesterol, and physical inactivity) have the same impact on men and women, the significance and the relative weighting of these factors are different in women during different life phases. Women with clinical manifestation of CAD are older than men, with a higher number of cardiovascular risk factors (clustering of risk factors). In addition, menopause is a watershed transition associated with a worsening CAD risk profile and acceleration of atherosclerosis.
Physical inactivity is one of the major risk factors responsible for increased chances of getting several other risk factors such as obesity, diabetes, hypertension, high cholesterol, and depression. Women in India are generally far more physically inactive than men, and this plays a significant role in future development of CAD. Regular exercise confers the same numerous health benefits to women as it does to men and it is one of the single most important preventive measures for all women, including postmenopausal women.
Body weight may increase during the 1st years since menopause and body fat distribution changes from a gynoid to a more android pattern. Central obesity with an increase in visceral fat occurs more frequently after menopause, with a higher presence of comorbid risk factors and components of the metabolic syndrome in women compared with aging men.[17] With the increasing incidence of obesity, there is a parallel increase in the prevalence of type 2 diabetes.
Women with diabetes are at greater risk for cardiovascular complications than their male counterparts. In a meta-analysis of 37 prospective cohort studies, the risk of fatal CHD is 50% higher in women with diabetes compared with male diabetics.[18]
Systolic blood pressure rises more steeply in aging women compared with men, and this may be related to the decline in estrogen levels in menopause transition.[19,20,21] At older age (>75 years), isolated systolic hypertension is 14% more prevalent in women and an important cause of left ventricular hypertrophy, diastolic heart failure, and strokes. Moderate or borderline hypertension (<140/90 mmHg) causes more endothelial dysfunction and cardiovascular complications in women than in men.[22]
At younger age, the relative risk of hyperlipidemia is lower in women compared to men. However, in postmenopausal women, total cholesterol and low-density lipoprotein (LDL) levels rise by 10% and 14%, respectively, and lipoprotein (a) increases 4%–8%, whereas HDL cholesterol levels remain unchanged.[23] From the Framingham study, it is known that low HDL cholesterol implicates a higher CHD risk in women than in men.[24] Although women have often been underrepresented in many statin trials in the past, there is currently no doubt that in secondary prevention, LDL reduction in women leads to an equally lower CHD mortality as in men.[25] For primary prevention, the role of statin and aspirin therapy in women is still controversial, except perhaps in diabetic women with multiple CAD risk factors.
TOBACCO CONSUMPTION IN WOMEN
Women are more prone to develop tobacco-induced atherothrombosis compared to men. In India, 47% of men and 14% of women either smoked or chewed tobacco.[24] Tobacco consumption (bidi/gutkha/paste) was significantly higher in poor, less educated, and scheduled castes and scheduled tribe populations, while smoking was more prevalent in higher socioeconomic and educated populations.
Therefore, prevention and management of CVD in women should begin with early and increased awareness of the problem and better understanding of the disease's unique characteristics in women. Recent trend to identify female-specific risk factors and/or clustering of risk factors for CAD at younger age and to utilize them in risk stratification makes it more effective to identify premenopausal women at higher future risk for CAD. Applying earlier and more aggressive preventive measures such as lifestyle changes of regular exercise and healthy diet along with pharmacological options for tighter control of diabetes, hypertension, and lipids can play a crucial role in reducing the CAD incidence and mortality in later life in this subset of women.
The sex/gender differences in the burden of CVD and coronary heart disease (CHD), from the Heart Disease and Stroke Statistics, American Heart Association, are depicted in Table 2.
Table 2.
Sex/gender differences in the burden of cardiovascular disease
| Men | Women | |
|---|---|---|
| Remaining lifetime risk for CVD at age 40 y | 2 in 3 | 1 in 2 |
| CVD | ||
| Deaths caused by CVD and congenital heart disease (2007), n | 391 886 | 421 918 |
| Age-adjusted CVD death rate per 100 000 (2007) | 300.3 | 211.6 |
| Prevalence of CVD (2008, age ≥20 y), n (%) | 39 900 000(37.4) | 42 700 000(35.0] |
| Hospital discharges for CVD (2007) | 3016 000 | 2 874 000 |
| CHD | ||
| Deaths caused by CHD (2007), n | 216 050 | 190 301 |
| Age-adjusted CHD death rate per 100 000 (2007) | 165.4 | 95.7 |
| Prevalence of CHD (2008, age≥20 y), n (%) | 8 800 000(8.3) | 7 500 000(6.1) |
| Prevalence of angina pectoris (2008, age≥20 y), n (%) | 4 000 000(3.8) | 5 000 000(4.0) |
| Hospital discharges for CHD (2007), n | 965 000 | 607 000 |
| Stroke | ||
| Deaths resulting from stroke (2007, all ages) | 54111 | 81 841 |
| Age-adjusted stroke death rate per 100000 | 42.5 | 41.3 |
| Prevalence of stroke (2008, age 220 y), n (%) | 2 800 000(2.7) | 4 200 000(3.3) |
| Hospital discharges for stroke (2007), n | 371 000 | 458 000 |
| Heart failure | ||
| Prevalence of heart failure (2008, age≥20 y), n (%) | 3100 000(3.0) | 2 600 000(2.0) |
| Hospital discharges for heart failure (2007, all ages) | 470 000 | 520 000 |
| Economic burden | ||
| Percent in-hospital patient cost | 51.7 | 48.3 |
| Percent of $187 billion national cost | 57.2 | 42.8 |
Source: Heart disease and stroke statistics, American Heart Association[40]. CVD: Cardiovascular disease, CHD: Coronary heart disease
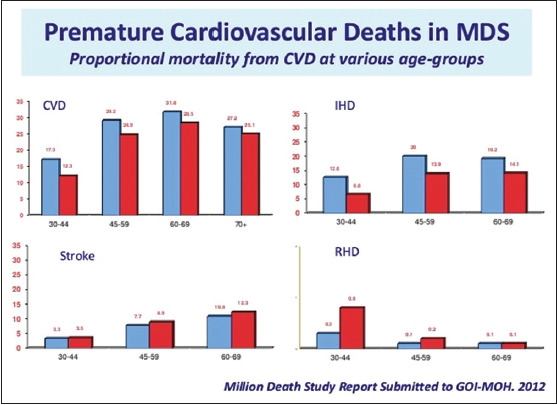
The high total mortality due to CVD in men and women in India is shown in Table 3A, and the subgroup analysis of different causes of CVD mortality is given in Table 3B as per the Million Death Study 2012.
Table 3A.
CVD Mortality
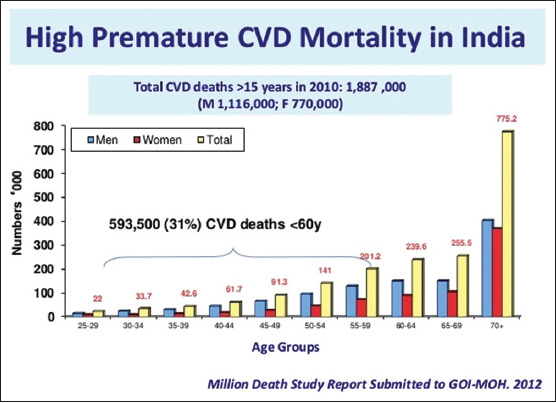
Table 3B.
Cardiovascular Deaths
GENDER DIFFERENCES IN CLINICAL PRESENTATION AND INTERPRETATIONS OF NONINVASIVE TESTING
There has long been a perception that angina symptoms in women are somewhat different than in men. Both women and men use the terms such as “chest pain,” “pressure,” and “tightness.” Men tend to describe angina as “chest pain,” while women use words such as “heaviness” to explain what they are feeling and often they are late in reporting the symptoms. In addition to the more common chest pain, there are less common signs that may signal angina. These include unusual shortness of breath, unusual fatigue, unexpected sweating, and unexplained weakness. Symptoms more commonly described by women have been dubbed as “atypical angina” but many women “are really exhibiting typical angina symptoms“. This means acknowledging the possibility of angina no matter how a women describes suspicious chest-related symptoms.[26,27,28]
Lower self-awareness among women and lower social priority also are important contributors of higher CVD mortality in women.[19] Like the clinical presentation, the interpretation of noninvasive diagnostic testing is also less reliable in women compared with men, especially in the age group below 55 years when the prevalence of CAD is still relatively low.
THE INDIVIDUAL ROLE OF INVESTIGATIONS
Resting electrocardiography (ECG) may show nonspecific ST-T changes, and ECG interpretation often is difficult in women. Although a useful test, exercise ECG test (TMT) can be less sensitive and less specific for a diagnosis in women. Nonspecific ECG changes at rest, a lower exercise capacity, and a smaller vessel size contribute to the lower sensitivity and specificity of noninvasive testing in women.[29] Stress echocardiography (with exercise or dobutamine) can be a useful test having no significant gender difference in interpretation. Microvascular dysfunction and diffuse coronary atherosclerosis without obstructive lesions in major epicardial arteries are more prevalent in women than in men and can be better visualized with positron emission tomography (PET) and cardiovascular magnetic resonance (CMR) techniques.[30,31]
CT coronary calcium score[32] can be a valuable noninvasive test for women aged >50 years with intermediate risk (those having one or more of the risk factors such as hypertension, diabetes, dyslipidemia, family history of CAD, central obesity, and tobacco/smoking history) or in symptomatic women with ambiguous ECG/stress test results to rule out presence of CAD. Absence of coronary calcium (calcium score zero) has 99% negative predictive value. However, it must be noted that calcium scores are somewhat lower in women than men at any age.[32] As per the findings of The Multi-Ethnic Study of Atherosclerosis published May 6, 2014, Circulation, the presence of calcium deposits (CT calcium score >100) in coronaries establishes the presence of atheromatous plaques and the need to prescribe statins and aspirin even in absence of CAD symptoms. The coronary computed tomographic angiography (CCTA), although a less desirable test for younger women due to its high radiation exposure, can be a very useful test in nonpregnant women <65 years who present with acute chest pain at the emergency department.[33]
All these facts implicate that traditional diagnostic methods are not optimal for women, and regardless of this ambiguity, women with symptoms suggestive of CAD should be investigated and treated more aggressively including their risk factors. It is important to remember that women who are diagnosed with noncardiac chest pain have a twofold increased risk to develop a CHD event in the next 5–7 years and have a four times higher risk for re-hospitalizations and recurrent angiograms in the next 180 days.[34,35,36]
ACUTE CORONARY SYNDROME AND ITS MANAGEMENT IN WOMEN
At a presentation in ST elevation MI (STEMI), both men and women have comparable symptoms of chest pain, but women tend to have more concomitant vaso-vegetative symptoms that can mask the chest pain with less extensive ST-T elevations at admission, especially at younger age.[14,37,38] In women below 55 years of age, unstable angina pectoris and non-STEMI are often misdiagnosed at the emergency department.[39] Women with ACS are generally older with more clustering of risk factors that may contribute to their higher risk of mortality.[14,15,40] Gender bias in treatment and gender disparities in vascular flow and structure may further add to this increased mortality.
CHEST PAIN WITH “NORMAL” CORONARY ANGIOGRAMS
When symptoms of microvascular dysfunction result in objective signs of ischemia (ST changes in ECG or ECHO findings of hypokinesis), it is proposed to call this as syndrome X or syndrome of microvascular angina. Such women need and respond well to treatment with coronary vasodilators, calcium blockers, nicorandil, and trimetazidine-like agents. The relationship between microvascular dysfunction and epicardial atherosclerosis is not yet fully understood. The prognosis of this syndrome is less favorable than initially considered and often leads to recurrent hospitalizations and repeated coronary angiograms.[34,35] The prognosis is worse in women with multiple risk factors and they should be treated aggressively to prevent future CHD events.
MANAGEMENT OF ACUTE CORONARY SYNDROMES
While in STEMI, both genders have equal benefit of early percutaneous coronary interventions (PCI), in non-STEMI, an early conservative strategy in low risk (bio-marker negative) women is better than early invasive strategy.[41] Mortality after coronary artery bypass surgery (CABG) is higher in women compared with men and this difference is more pronounced in the younger age groups, after adjustment for risk factors.[42]
Currently, there are limited data regarding sex differences in the presentation, management, and outcomes of acute manifestations of noncommunicable, chronic diseases in India, particularly CVD. In an analysis using the Kerala ACS Registry, the largest prospective ACS registry in India containing 25,748 ACS admissions, even though women with ACS were older and more likely to have previous myocardial infarction, there were no significant differences found in in-hospital and discharge management, in-hospital mortality, or major adverse cardiovascular events between sexes.[43] In a recent Indian study done by Gurram et al., 2019,[44] women were not found to be having higher short term mortality postbypass surgery. In another study pertaining to find out gender difference in long-term outcome of bypass surgery, it was found that both male and female patients improve in physical, social, and emotional functioning after CABG, and recovery over time is similar in men and women. However, women's health-related quality-of-life scale scores remained less favorable than men's through 1 year after surgery.[45]
PREVENTIVE MEASURES
A greater public health awareness and improved medical practitioners' knowledge regarding gender-based differences in CAD can play a crucial role in adopting a proactive strategy of early prevention, detection, and management of CAD in younger women resulting in lower incidence of CAD and better treatment outcomes in later life [Table 4].[46]
Table 4.
Cardiovascular disease prevention in women: What we have learned in the past decade
| Unknown in 2000 | Known in 2011 |
|---|---|
| Does MHT prevent incident CVD? | MHT does not prevent incident or recurrent CVD and increases risk of stroke in susceptible patients. MHT is safe in women without established CVD or are at low to moderate risk for CVD |
| Do SERMs prevent incident or recurrent CVD? | SERMs do not prevent incident or recurrent CVD in women and increase risk of fatal stroke and VTE |
| Is aspirin effective for the primary prevention of CVD in women? | Aspirin does not prevent incident MI in women <65 years; aspirin prevents recurrent CVD and incident ischemic stroke and might prevent incident MI in women <65 years of age but increases risk of hemorrhagic strokes and GI bleeding |
| Do antioxidant supplements prevent incident or recurrent CVD? | Vitamins E and C and beta carotene do not prevent incident or recurrent CVD |
| Do folic acid and B vitamin supplements prevent incident or recurrent CVD? | Folic acid and B vitamin supplements do not prevent incident or recurrent CVD |
| Does omega-3 fatty acid supplementation prevent incident or recurrent CVD? | Omega-3 might prevent CVD in women with hypercholesterolemia but the absolute benefit is low |
| Does vitamin D and calcium supplementation prevent incident or recurrent CVD? | Combined vitamin D (400 IU daily) and calcium supplementation (1000 mg/d) do not increase CVD risk, stroke, or mortality |
| Does intensive diabetic control prevent CVD? | Targeting HbA1C<6% does not prevent CVD events in patients with diabetes mellitus and increases the risk of death |
| Is LDL reduction effective for the primary prevention of CVD in women? | LDL reduction reduces recurrent events and might reduce incident events in women, but the absolute benefit for primary prevention is small[41] |
CVD: Cardiovascular disease, SERMs: Selective estrogen receptor modulators, LDL: Low-density lipoprotein, MHT: Menopausal hormone therapy, VTE: Venous thromboembolism, MI: Myocardial infarction, GI: Gastrointestinal, HbA1C: Hemoglobin A1C
Physical activity is a proven means of primary prevention of not only CVD but also disease risk factors for CVD such as diabetes, hypertension, and obesity. Lack of physical activity was evident in our study population. Women who did not walk or cycle as a regular means of transport had one and a half times greater chance of high CVD risk.
Single/separated/widowed women were nearly twice more likely to have high CVD risk as compared to married women. This suggests a lack of financial and social support, which are barriers to healthy eating. Appropriate counseling services and stress management program for such women can play a crucial role in prevention.[46]
CONCLUSION
Despite women's high lifetime risk of dying from CVD and higher prevalence of angina, there remains a perception that CVD is a “Man's disease.” Over the past half century, this misperception has led to the underappreciation, underrecognition, and underdiagnosis of CVD in women, resulting in less medical therapy and fewer invasive procedures compared with men.
Gender-based variations in presentation sign/symptoms; ECG/TMT interpretations; and even coronary angiographic findings (microvessel disease) together with gender differences of various hormonal, vascular, and biological factors lead to misdiagnosis or delayed treatment, and as a result, women remain at higher risk of getting CV events and deaths.
The recent trend to identify female-specific risk factors for CAD and to utilize them in risk stratification makes it easier to identify premenopausal women at higher future risk for CAD. Applying earlier and more aggressive preventive measures such as exercise and lifestyle changes along with pharmacological options to tightly control major risk factors such as diabetes, hypertension, and high lipids can play a crucial role in reducing the CAD incidence and mortality in later life in this subset of women.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Mohan V, Deepa R, Rani SS. Prevalence of coronary artery disease and its relationship to lipids in a selected population in South India. J Am Coll Cardiol. 2001;38:682–7. doi: 10.1016/s0735-1097(01)01415-2. [DOI] [PubMed] [Google Scholar]
- 2.Gupta R, Gupta VP, Sarna M. Prevalence of coronary heart disease and risk factors in an urban Indian population: Jaipur Heart Watch-2. Indian Heart J. 2002;54:59–66. [PubMed] [Google Scholar]
- 3.Kamili M, Dar I, Ali G, Wazir H, Hussain S. Prevalence of coronary heart disease in Kashmiris. Indian Heart J. 2007;59:44–9. [PubMed] [Google Scholar]
- 4.Gupta AK, Bharadwaj A, Ashotra S. Feasibility and training of multipurpose workers in detection, prevention and control of coronary artery disease in apple-belt of Shimla hills. South Asian J Prev Cardiol. 2002;6:17–22. [Google Scholar]
- 5.Kumar R, Singh MC, Singh MC, Ahlawat SK, Thakur JS, Srivastava A, et al. Urbanization and coronary heart disease: A study of urban-rural differences in northern India. Indian Heart J. 2006;58:126–30. [PubMed] [Google Scholar]
- 6.Yusuf S, Hawken S, Ounpuu S. The INTERHEART study investigators effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART Study): Case control study. Lancet. 2004;364:937–52. doi: 10.1016/S0140-6736(04)17018-9. [DOI] [PubMed] [Google Scholar]
- 7.Dasgupta S, Salman M, Lokesh S, Xaviour D, Yaseen Saheb S, Ravi Prasad BV, et al. Menopause versus aging: The predictor of obesity and metabolic aberrations among menopausal women of Karnataka, South India. J Midlife Health. 2012;3:24–30. doi: 10.4103/0976-7800.98814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pandey S, Srinivas M, Agashe S, Joshi J, Galvankar P, Prakasam CP, et al. Menopause and metabolic syndrome: A study of 498 urban women from western India. J Midlife Health. 2010;1:63–9. doi: 10.4103/0976-7800.76214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mehndiratta N, Sharma S, Sharma RK, Grover S. A prospective study on the incidence of metabolic syndrome in premenopausal and postmenopausal women. J Midlife Health. 2020;11:17–21. doi: 10.4103/jmh.JMH_57_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kirtikar U, Kajale N, Patwardhan V, Khadilkar V, Khadilkar AV. Cardiometabolic risk in pre- and post-menopausal women with special reference to insulin resistance: A cross-sectional study. J Midlife Health. 2020;11:22–6. doi: 10.4103/jmh.JMH_65_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sharma S, Aggarwal N, Joshi B, Suri V, Badada S. Prevalence of metabolic syndrome in pre- and post-menopausal women: A prospective study from apex institute of North India. J Midlife Health. 2016;7:169–74. doi: 10.4103/0976-7800.195695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Manjareeka M, Nanda S, Mishra J, Mishra S. Correlation between anthropometry and lipid profile in healthy subjects of Eastern India. J Midlife Health. 2015;6:164–8. doi: 10.4103/0976-7800.172302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Khan Y, Lalchandani A, Gupta AC, Khadanga S, Kumar S. Prevalence of metabolic syndrome crossing 40% in Northern India: Time to act fast before it runs out of proportions. J Family Med Prim Care. 2018;7:118–23. doi: 10.4103/jfmpc.jfmpc_10_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hochman JS, Tamis JE, Thompson TD, Weaver WD, White HD, Van de Werf F, et al. Sex, clinical presentation, and outcome in patients with acute coronary syndromes. Global Use of Strategies to Open Occluded Coronary Arteries in Acute Coronary Syndromes IIb Investigators. N Engl J Med. 1999;341:226–32. doi: 10.1056/NEJM199907223410402. [DOI] [PubMed] [Google Scholar]
- 15.Vaccarino V, Parsons L, Every NR, Barron HV, Krumholz HM. Sex-based differences in early mortality after myocardial infarction. National Registry of Myocardial Infarction 2 Participants. N Engl J Med. 1999;341:217–25. doi: 10.1056/NEJM199907223410401. [DOI] [PubMed] [Google Scholar]
- 16.Jacobs AK. Coronary intervention in 2009. Are women no different than men? Circ Cardiovasc Intervent. 2009;2:69–78. doi: 10.1161/CIRCINTERVENTIONS.108.847954. [DOI] [PubMed] [Google Scholar]
- 17.Kip KE, Marroquin OC, Kelley DE, Johnson BD, Kelsey SF, Shaw LJ, et al. Clinical importance of obesity versus the metabolic syndrome in cardiovascular risk in women: A report from the Women's Ischemia Syndrome Evaluation (WISE) study. Circulation. 2004;109:706–13. doi: 10.1161/01.CIR.0000115514.44135.A8. [DOI] [PubMed] [Google Scholar]
- 18.Huxley R, Barzi F, Woodward M. Excess risk of fatal coronary heart disease associated with diabetes in men and women: Meta-analysis of 37 prospective cohort studies. BMJ. 2006;332:73–8. doi: 10.1136/bmj.38678.389583.7C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Burt VL, Whelton P, Roccella EJ, Brown C, Cutler JA, Higgins M, et al. Prevalence of hypertension in the US adult population. Results from the Third National Health and Nutrition Examination Survey, 1988-1991. Hypertension. 1995;25:305–13. doi: 10.1161/01.hyp.25.3.305. [DOI] [PubMed] [Google Scholar]
- 20.Dubey RK, Oparil S, Imthurn B, Jackson EK. Sex hormones and hypertension. Cardiovasc Res. 2002;53:688–708. doi: 10.1016/s0008-6363(01)00527-2. [DOI] [PubMed] [Google Scholar]
- 21.Barton M, Meyer MR. Postmenopausal hypertension: Mechanisms and therapy. Hypertension. 2009;54:11–8. doi: 10.1161/HYPERTENSIONAHA.108.120022. [DOI] [PubMed] [Google Scholar]
- 22.Vasan RS, Larson MG, Leip EP, Evans JC, O’Donnell CJ, Kannel WB, et al. Impact of high-normal blood pressure on the risk of cardiovascular disease. N Engl J Med. 2001;345:1291–7. doi: 10.1056/NEJMoa003417. [DOI] [PubMed] [Google Scholar]
- 23.Abbey M, Owen A, Suzakawa M, Roach P, Nestel PJ. Effects of menopause and hormone replacement therapy on plasma lipids, lipoproteins and LDL-receptor activity. Maturitas. 1999;33:259–69. doi: 10.1016/s0378-5122(99)00054-7. [DOI] [PubMed] [Google Scholar]
- 24.Kannel WB, Castelli WP, Gordon T, McNamara PM. Serum cholesterol, lipoproteins, and the risk of coronary heart disease. The Framingham study. Ann Intern Med. 1971;74:1–2. doi: 10.7326/0003-4819-74-1-1. [DOI] [PubMed] [Google Scholar]
- 25.Rani M, Bonu S, Jha P, Nguyen SN, Jamjoum L. Tobacco use in India: Prevalence and predictors of smoking and chewing in a national cross sectional household survey. BMJ J Tob Control. 2003;12:e4. doi: 10.1136/tc.12.4.e4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Daly CA, Clemens F, Sendon JL, Tavazzi L, Boersma E, Danchin N, et al. The clinical characteristics and investigations planned in patients with stable angina presenting to cardiologists in Europe: From the Euro Heart Survey of Stable Angina. Eur Heart J. 2005;26:996–1010. doi: 10.1093/eurheartj/ehi171. [DOI] [PubMed] [Google Scholar]
- 27.Douglas PS, Ginsburg GS. The evaluation of chest pain in women. N Engl J Med. 1996;334:1311–5. doi: 10.1056/NEJM199605163342007. [DOI] [PubMed] [Google Scholar]
- 28.Johnson BD, Kelsey SF, Bairey Merz CN. Clinical risk assessment in women: Chest discomfort. Report from the WISE study. In: Shaw LJ, Redberg RF, editors. CAD in Women: Evidence-Based Diagnosis and Treatment. Totowa, NJ: Humana Press; 2003. pp. 129–42. [Google Scholar]
- 29.Mieres JH, Shaw LJ, Arai A, Budoff MJ, Flamm SD, Hundley G, et al. Role of non-invasive testing in the clinical evaluation of women with suspected coronary artery disease. Circulation. 2005;111:682–96. doi: 10.1161/01.CIR.0000155233.67287.60. [DOI] [PubMed] [Google Scholar]
- 30.Morise AP, Olson MB, Bairey Merz NC, Mankad S, Rogers WJ, Pepine CJ, et al. Validation of the accuracy of pretest and exercise test scores in women with a low prevalence of coronary disease: the NHLB sponsored Women's Ischemia Syndrome Evaluation (WISE) study. Am Heart J. 2004;147:1085–92. doi: 10.1016/j.ahj.2003.12.034. [DOI] [PubMed] [Google Scholar]
- 31.Reis SE, Holubkov R, Conrad Smith AJ, Kelsey SF, Sharaf BL, Reichek N, et al. Coronary microvascular dysfunction is highly prevalent in women with chest pain in the absence of coronary artery disease: Results from the NHLBI WISE study. Am Heart J. 2001;141:735–41. doi: 10.1067/mhj.2001.114198. [DOI] [PubMed] [Google Scholar]
- 32.Raggi P, Gongora MC, Gopal A, Callister TQ, Budoff M, Shaw LJ. Coronary artery calcium to predict all-cause mortality in elderly men and women. J Am Coll Cardiol. 2008;52:17–23. doi: 10.1016/j.jacc.2008.04.004. [DOI] [PubMed] [Google Scholar]
- 33.Shaw LJ, Bugiardini R, Bairey Merz CN. Women and ischemic heart disease. J Am Coll Cardiol. 2009;54:1561–75. doi: 10.1016/j.jacc.2009.04.098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Robinson JG, Wallace R, Limacher M, Ren H, Cochrane B, Wassertheil-Smoller S, et al. Cardiovascular risk in women with non-specific chest pain (from the Women's Health Initiative hormone trials) Am J Cardiol. 2008;102:693–9. doi: 10.1016/j.amjcard.2007.12.044. [DOI] [PubMed] [Google Scholar]
- 35.Humphries KH, Pu A, Gao M, Carere RG, Pilote L. Angina with “normal” coronary arteries: Sex differences in outcome. Am Heart J. 2008;155:375–81. doi: 10.1016/j.ahj.2007.10.019. [DOI] [PubMed] [Google Scholar]
- 36.Gulati M, Cooper-DeHoff RM, McClure C, Johnson BD, Shaw LJ, Handberg EM, et al. Adverse cardiovascular outcomes in women with nonobstructive coronary artery disease: A report from the Women's Ischemia Syndrome Evaluation Study and the St James Women Take Heart Project. Arch Intern Med. 2009;169:843–50. doi: 10.1001/archinternmed.2009.50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Milner KA, Funk M, Richards S, Wilmes RM, Vaccarino V, Krumholz HM. Gender differences in symptom presentation associated with coronary heart disease. Am J Cardiol. 1999;84:396–9. doi: 10.1016/s0002-9149(99)00322-7. [DOI] [PubMed] [Google Scholar]
- 38.Dey S, Flather MD, Devlin G, Brieger D, Gurfinkel EP, Steg PG, et al. Sex-related differences in the presentation, treatment and outcomes among patients with acute coronary syndromes: The Global Registry of Acute Coronary Events. Heart. 2009;95:20–6. doi: 10.1136/hrt.2007.138537. [DOI] [PubMed] [Google Scholar]
- 39.Pope JH, Aufderheide TP, Ruthazer R, Woolard RH, Feldman JA, Beshansky JR, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. N Engl J Med. 2000;342:1163–70. doi: 10.1056/NEJM200004203421603. [DOI] [PubMed] [Google Scholar]
- 40.Milcent C, Dormont B, Durand-Zaleski I, Steg PG. Gender differences in hospital mortality and use of percutaneous coronary intervention in acute myocardial infarction: Microsimulation analysis of the 1999 nationwide French hospitals database. Circulation. 2007;115:833–9. doi: 10.1161/CIRCULATIONAHA.106.664979. [DOI] [PubMed] [Google Scholar]
- 41.Donoghue MO, Boden W, Braunwald E, Cannon CP, Clayton TC, de Winter RJ, et al. Early invasive versus conservative treatment strategies in women and men with unstable angina and non-ST-elevation myocardial infarction. JAMA. 2008;300:71–80. doi: 10.1001/jama.300.1.71. [DOI] [PubMed] [Google Scholar]
- 42.Vaccarino V, Abramson JL, Veledar E, Weintraub WS. Sex differences in hospital mortality after coronary artery bypass surgery: Evidence for a higher mortality in younger women. Circulation. 2002;105:1176–81. doi: 10.1161/hc1002.105133. [DOI] [PubMed] [Google Scholar]
- 43.Patel A, Vishwanathan S, Mohanan PP. Sex differences in the presentation, diagnosis, and management of acute coronary syndromes. Glob Heart. 2015;10:273–80. doi: 10.1016/j.gheart.2015.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Gurram A, Krishna N, Vasudevan A, Baquero LA, Jayant A, Varma PK. Annals of cardiac anesthesia: Female gender is not a risk factor for early mortality after coronary artery bypass grafting. Journal of Annals of Cardiac Anesthesia. 2019;22:187–93. doi: 10.4103/aca.ACA_27_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kumar R, Hote MP, Sharma G, Thakur B, Airan B. Comparison of outcome in male and female Indian patients undergoing CABG, activity levels and quality of life: One year follow up study. Am J Thorac Cardiovasc Surg. 2017;2:29–34. [Google Scholar]
- 46.Raeisi-Giglou P, Volgman AS, Patel H, Campbell S, Villablanca A, Hsich E. Advances in Cardiovascular Health in Women overthe Past Decade: Guideline Recommendations for Practice. J Womens Health (Larchmt) 2018;27:128–39. doi: 10.1089/jwh.2016.6316. [DOI] [PMC free article] [PubMed] [Google Scholar]