

Abstract
Background:
Over 90,000 rescue and recovery responders to the September 2001 World Trade Center (WTC) attacks were exposed to toxic materials that can impair cardiac function and increase cardiovascular disease (CVD) risk. We examined WTC-related exposures association with annual and cumulative CVD incidence and risk over 17 years in the WTC Health Program (HP) General Responder Cohort (GRC).
Methods:
Post 9/11 first occurrence of CVD was assessed in 37,725 responders from self-reported physician diagnosis of, or current treatment for, coronary artery disease, myocardial infarction, stroke and/or congestive heart failure from WTCHP GRC monitoring visits. Kaplan–Meier estimates of CVD incidence used the generalized Wilcoxon test statistic to account for censored data. Cox proportional hazards regression analyses estimated the CVD hazard ratio associated with 9/11/2001 arrival in responders with and without dust cloud exposure, compared with arrival on or after 9/12/2001. Additional analyses adjusted for comorbidities.
Results:
To date, 6.3% reported new CVD. In covariate-adjusted analyses, men’s CVD 9/11/2001 arrival risks were 1.40 (95% confidence interval [CI] = 1.26, 1.56) and 1.43 (95% CI = 1.29, 1.58) and women’s were 2.16 (95% CI = 1.49, 3.11) and 1.59 (95% CI = 1.11, 2.27) with and without dust cloud exposure, respectively. Protective service employment on 9/11 had higher CVD risk.
Conclusions:
WTCHP GRC members with 9/11/2001 exposures had substantially higher CVD risk than those initiating work afterward, consistent with observations among WTC-exposed New York City firefighters. Women’s risk was greater than that of men’s. GRC-elevated CVD risk may also be occurring at a younger age than in the general population.
Keywords: cardiovascular disease, environmental exposure, occupation, responder/recovery worker, World Trade Center
1 |. INTRODUCTION
Heart disease continues to be the leading cause of death worldwide,1–3 only recently surpassed by cancer among middle-aged people in the United States and other high-income countries.4 Major risk factors include older age, cigarette smoking, diet and obesity, high blood pressure, high cholesterol, diabetes, and work psychosocial stressors.1–3,5–7 In some studies,8–14 exposure to air pollution, radioactive materials, some environmental toxic metals, and other particulate matter have been associated with cardiac function damage and increased risk of heart disease and death. Others have found null or negative associations of such exposures with cardiovascular risk and disease, and this lack of association is sometimes attributed to a healthy worker effect.15–18
In response to the 9/11/2001 terrorist attacks on the World Trade Center (WTC), more than 90,000 people participated in rescue and recovery efforts and in debris cleanup.19,20 These responders were exposed to a complex mix of toxins, including burning jet fuel from the hijacked airplanes and hazardous particulate matter from the collapse of the WTC towers.21,22 In addition to physiologic stress, many responders experienced work psychosocial stressors that can initiate or exacerbate unhealthy chronic biologic processes and behavioral responses and influence CVD risk.7,23 These exposures have been associated with increased short-term and persistent risk of morbidity, including respiratory disease, gastro–esophageal reflux disorder, posttraumatic stress disorder (PTSD), and certain cancers.20,24–26
An analysis of WTC Registry responders and non-responders through 2009 who had high levels of exposure were found to have death rates from heart disease that were more than twice the rates observed in those with less exposure to the environmental site contaminants.27 By 2014, female WTC Registry members who had intense dust cloud exposure had a 1.28 times higher risk of physician-diagnosed heart disease than less exposed women (95% confidence interval [CI] = 1.02, 1.61), whereas men with intense dust cloud exposure had a 1.14 (95% CI = 0.97, 1.34) times higher rate of physician-diagnosed heart disease than men with less exposure.28 In an early 4-year responder follow-up, higher risks for PTSD-mediated heart attack and stroke were observed in surviving responders involved in debris cleanup.29 For the earliest arriving firefighter responders, who were exposed to the toxic dust cloud on 9/11/2001, a 1.44 (95% CI = 1.09, 1.90) higher risk of primary cardiovascular disease (CVD) was observed compared with responders who had less toxic exposure arriving on or after 9/12/2001.30
Using 17 years of follow-up of the WTC Health Program’s (HP) large, diverse General Responder Cohort (GRC) of both men and women, this study’s objective was to examine the annual and cumulative incidence of CVD. We also investigated the association of CVD risks with 9/11/2001 exposures, based on whether or not the responders reported being exposed to the dust cloud, compared with those arriving on or after 9/12/2001.
2 |. MATERIALS AND METHODS
This study was conducted in adherence to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidance.
2.1 |. Study population
The WTCHP GRC is an open (continuing to enroll) cohort. Through March 31, 2019, 32,539 men and 5186 women general responders who reported whether they had or had not been diagnosed with or treated for CVD have been followed.
2.2 |. WTCHP GRC eligibility criteria and recruitment
The WTCHP GRC recruited its participants using publicity and broad outreach through various mechanisms (volunteers, community and labor organizations; governmental and legislative agencies and media). Men and women eligible for the WTCHP GRC include those who worked or volunteered at the tower sites in lower Manhattan, at the Staten Island landfill or on certain barge-loading piers for at least 4 h between September 11 and 14, 2001, who worked at least 24 h between September 11 and 30, 2001 or at least 80 h between September 11 and July 31, 2002. The WTCHP GRC comprises rescue and recovery workers and volunteers who were enrolled in the HP on or after July 16, 2002.31 This includes staff who had contact with WTC-related human remains from the Office of the Chief Medical Examiner between September 11, 2001 and July 31, 2002, and those from the Port Authority Trans-Hudson Corporation who cleaned tunnels for at least 24 h between February 1, 2002 and July 1, 2002.32 Other responders who may not be included in the WTCHP GRC are employees of the Fire Department of the City of New York (FDNY), individuals participating in the New York City Department of Health Registry (~23% also participate in the WTCHP GRC), Pentagon and Shanksville responders, Nationwide Provider Network members (not WTCHP GRC participants), and others participating and not participating in similar programs.20,28
2.3 |. Data collection
Responders voluntarily participating in the program were first interviewed (beginning July 2002) to assess their socio-demographic characteristics and WTC-related exposures, after which they received a comprehensive, standardized physical and mental health examination. Program participants were subsequently interviewed and examined every 12–18 months, depending upon their presentation for program visits. The data were collected, using a standardized clinical interview, from each WTCHP GRC participant at each monitoring visit from July 16, 2002. Data available at the time of analysis, through March 31, 2019, were analyzed.
2.4 |. Data source
CVD was defined as a responder’s self-report of a physician’s first diagnosis or responders’ reporting that they were under current treatment for first-time coronary artery disease (CAD), myocardial infarction (MI), stroke, or congestive heart failure (CHF). Only monitoring visit reports of diagnosis or treatment on or after 9/11/2001 are classified as having post 9/11 CVD. Responders were classified as not having post 9/11 CVD if they did not report a physician diagnosis or treatment for any of these conditions. Additionally, reported heart murmur and other heart diseases were not included in the definition of CVD. Individuals solely reporting heart murmur or other heart diseases were retained as noncases in the analysis.
Exposure was categorized by self-report as follows: first arrival at the WTC site on 9/11/2001 reporting exposure to the dust cloud (very high exposure); first arrival on 9/11/2001 not reporting exposure to the dust cloud (high exposure); and first arrival on or after 9/12/2001 (low/intermediate exposure).
2.5 |. Statistical analyses
We conducted analyses to compare the effects of more intense (very high and high) with less intense (low/intermediate) WTCHP GRC exposures. The conditional cumulative incidence of post 9/11 first-time CVD was assessed by Kaplan–Meier analyses, using the generalized Wilcoxon test statistic to account for censored data. Responders with pre-existing (before 9/11/2001) CVD were excluded from this evaluation to ensure any association with WTC exposure was not attributable to prior CVD history (n = 302). Age-to-diagnosis, which simultaneously adjusts for time since 9/11 and age at 9/11, was estimated as the age at the reported earliest post 9/11 date of a physician’s diagnosis of CAD, MI, stroke, or CHF and 9/11/2001.33 As the analysis includes a maximum of 17 years’ follow-up, results were censored at the most recent follow-up fewer than 17 years before March 31, 2019. The annual incidence was calculated as each year’s difference in cumulative incidence. Cox proportional hazards regression analyses were conducted to estimate the risk of CVD associated with high and very high exposure compared with low/intermediate exposure. As men constitute the large majority of WTCHP GRC and their results were almost identical to the total sample results, adjusted Cox proportional hazards regression analyses were conducted stratified by responders’ sex. To determine the influence of potential confounders, covariate-adjusted analyses included race/ethnicity. Additional Cox proportional hazards models included comorbidities and risk factors that could have been influenced by their WTC exposure and are in the causal pathway for CVD. These variables include self-reported lifetime cigarette smoking, cholesterol, hypertension, and diabetes status, and measured initial visit body mass index (BMI). Cigarette smoking was classified as never (the referent value), former, or current smoker. Height and weight were measured at each visit. Initial visit BMI was calculated as 703 × measured weight in pounds/(measured height in inches)2 and then categorized as <25 (normal), 25 to <30 (overweight), ≥30 (obese). At each monitoring visit, responders reported whether they had ever been diagnosed with high cholesterol, hypertension, and diabetes. Associations with these comorbidities, (not having high cholesterol, hypertension, or diabetes, respectively, are the referent groups), were examined in the comorbidity-adjusted analyses as risk factors in the causal pathway of WTC exposure and CVD. Because the responders’ reported dates were frequently missing for the first physician diagnosis of high cholesterol, high blood pressure, and/or diabetes; their categories are reported as “ever or never diagnosed” and do not reflect cases solely diagnosed before the first CVD date of diagnosis.
Being employed in high-stress occupations has been associated as a CVD risk factor.34,35 As over half of the WTCHP GRC were engaged in the high-stress occupation of protective services on 9/11, sensitivity analyses were conducted to evaluate whether protective services occupation on 9/11/2001 influenced the observed results. Cross-tabulations were conducted to determine whether the proportion of those actively engaged in protective services varied by WTC 9/11 arrival time with and without self-reported exposure to the dust cloud, and dichotomous variables were added to the Cox regressions to assess their associations with CVD risk and how 9/11 protective services occupation influenced the effects of WTC 9/11 exposures. Further analyses were conducted by including, in the statistical models, diagnosis of cancer since 9/11/2001, and unknown cancer status before CVD as proxies for having potentially received cancer treatment that may have increased the risk of CVD.36 To assess recall bias, we also examined whether the age of reported CVD diagnosis was influenced by when the WTCHP GRC participants enrolled in the health monitoring program.
All variables calculated using dates imputed missing days as each month’s midpoint, missing month as June, and missing year only when information from a consecutive visit could clarify the missing year. Missing covariate values were recoded to the sex-specific mode value in the multivariate analyses, which was the referent value of zero except for high cholesterol, BMI, and occupation on 9/11. For consistency with the other comorbidities (and because nearly 50% of men and women reported ever being diagnosed or treated for high cholesterol), missing data for high cholesterol was set to the referent value of zero for both sexes. Missing BMI was set to obese for men and overweight for women. For the sensitivity analyses for protective services, missing occupation was conservatively coded as the referent value of ‘not protective services.’
The Cox proportional hazards assumption was assessed via Schoenfeld residuals. No violations were found for the primary factors of interest except in the comorbidity-adjusted sensitivity analyses for protective services. Sensitivity analysis adding log survival time interactions for the violating covariates and comorbidities was used to address the variables where proportionality was violated. Analyses included all WTCHP GRC who provided written voluntary consent for research data aggregation and who presented for at least one monitoring visit. In addition to the previously mentioned exclusions, responders with unknown arrival date on the WTC site or unknown dust cloud exposure (n = 1005); and responders with unknown sex (n = 1) or age (n = 1) were also excluded from the analysis.
Descriptive statistics were conducted using SPSS 24.0 (IBM Corp.). The Cox proportional hazards analyses and Schoenfeld tests of the proportional hazards models were conducted in Stata (StataCorp. 2019, Stata Statistical Software: Release 16; StataCorp LLC.).
3 |. RESULTS
This analysis includes 37,725 WTCHP GRC, 86% male (Table 1). Most were between 30 and 59 years old with a median age of 37 (ranging from 19 to 80) years old on 9/11/2001. Most of the responders were married, white non-Hispanic, never smoked cigarettes, and employed in protective services on 9/11/2001. Half the participants enrolled in the WTCHP GRC before 2008, another 25% enrolled between 2008 and 2013, and 25% enrolled after 2013. Those enrolled before 2008 have participated in 6 ± 4 health monitoring visits (range, 1–14), and those enrolled between 2008 and 2013 have participated in 5 ± 3 (range, 1–11) visits. Those enrolled in 2014 and after have participated in 2 ± 2 health monitoring visits. Twenty-one percent have made only one health monitoring visit, 53% of whom enrolled in 2014 or after, 32% of whom enrolled before 2008, and 14% of whom enrolled between 2008 and 2013. Nineteen percent first arrived at the WTC site on 9/11/2001 and reported being exposed to the toxic dust cloud (men: 19.5%, women: 16.2%); 25.6% arrived on 9/11/2001 and reported that they were not exposed to the dust cloud (men: 26.2%; women: 22.3%); and 55.3% (men: 54.3%; women: 61.5%) arrived on or after 9/12/2001.
TABLE 1.
WTCHP GRC participant characteristics (n = 37,725)
| N | % | |
|---|---|---|
| Age (years) on 9/11/2001 | ||
| 20–29 | 1153 | 3.1 |
| 30–39 | 8871 | 23.5 |
| 40–49 | 15,021 | 39.8 |
| 50–59 | 9188 | 24.4 |
| 60+ | 3492 | 9.3 |
| Sex | ||
| Male | 32,539 | 86.3 |
| Female | 5186 | 13.7 |
| Race/ethnicity | ||
| White | 20,241 | 53.7 |
| Black | 3422 | 9.1 |
| Asian | 464 | 1.2 |
| Hispanic | 6992 | 18.5 |
| Other, not reported | 6606 | 17.5 |
| Cigarette smoker | ||
| Never | 21,754 | 57.7 |
| Former | 9713 | 25.7 |
| Current | 2651 | 7.0 |
| Missing | 3607 | 9.6 |
| Occupation on 9/11/2001 | ||
| Protective services/military | 19,968 | 52.9 |
| Construction | 6601 | 17.5 |
| Electrical, telecom, and other installation and repair | 2463 | 6.5 |
| Transportation and material moving occupations | 2008 | 5.3 |
| Other jobs | 4744 | 12.6 |
| Unemployed/retired | 516 | 1.4 |
| Not reported | 1425 | 3.8 |
| Marital status on 9/11/2001 (n = 37,434) | ||
| Single | 4184 | 11.1 |
| Married or partnered | 27,084 | 71.8 |
| Separated or divorced | 5539 | 14.7 |
| Widowed | 627 | 1.7 |
| Missing | 291 | 0.8 |
| Initial body mass index (703 × pounds/inches2) | ||
| <25 (normal) | 5263 | 14.3 |
| 25 to <30 (overweight) | 15,373 | 41.8 |
| ≥30 | 16,146 | 42.8 |
| Missing | 943 | 2.5 |
| Ever diagnosed with diabetes | 5193 | 13.8 |
| Missing | 125 | 3.3 |
| Ever diagnosed with high cholesterol | 19,672 | 52.1 |
| Missing | 4099 | 10.9 |
| Ever diagnosed with high blood pressure | 16,167 | 42.9 |
| Missing | 155 | 0.4 |
| WTCHP GRC exposure based on arrival at site | ||
| On or after 9/12 | 20,866 | 55.3 |
| On 9/11, not dust cloud | 9673 | 25.6 |
| On 9/11, in dust cloud | 7186 | 19.0 |
| Year of WTCHP GRC enrollment | ||
| ≤2007 | 18,874 | 50.0 |
| 2008–2013 | 9231 | 24.5 |
| ≥2014 | 9620 | 25.5 |
Abbreviations: GRC, General Responder Cohort; WTCHP, World Trade Center Health Program.
To date, 6.3% (n = 2385) of WTCHP GRC reported having been diagnosed with or treated for first-time CVD (Table 2). More than half of the reported CVD cases are CAD (3.8%), followed by stroke (1.8%), MI (1.3%), and CHF (0.7%). While male and female responders’ prevalence of post 9/11 stroke and CHF are similar, men’s prevalence of CAD and MI are nearly three times that of women. The mean age at CVD diagnosis was 52.4 ± 9.0 years, with an average of 7.9 ± 4.7 years since 9/11/2001 when diagnosed. The age and years since 9/11/2001 at diagnosis did not vary by sex; there was also little variation in age at diagnosis across CVD conditions.
TABLE 2.
CVD (CAD, MI, stroke, CHF) prevalence in WTCHP GRCa
| Diagnosed on/after 9/11 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Men (n = 32,539) | Women (n = 5186) | Total (n = 37,725) | |||||||
| N | % | Age at diagnosis; mean (SD) | N | % | Age at diagnosis; mean (SD) | N | % | Age at diagnosis; mean (SD) | |
| Coronary artery disease | 1360 | 4.2 | 53.2 (8.6) | 81 | 1.6 | 53.1 (9.9) | 1441 | 3.8 | 53.2 (8.7) |
| Heart attack (MI) | 476 | 1.1 | 52.3 (7.6) | 26 | 0.5 | 54.4 (10.2) | 502 | 1.3 | 52.4 (7.8) |
| Stroke | 586 | 1.8 | 52.8 (9.6) | 84 | 1.6 | 51.2 (10.6) | 670 | 1.8 | 52.6 (9.7) |
| Congestive heart failure | 226 | 0.7 | 51.3 (10.1) | 27 | 0.5 | 49.5 (10.6) | 253 | 0.7 | 51.2 (10.2) |
| Total reporting ≥1 CVD | 2192 | 6.7 | 52.5 (8.8) | 193 | 3.7 | 51.8 (10.4) | 2385 | 6.3 | 52.4 (9.0) |
Abbreviations: CAD, coronary artery disease; CHF, congestive heart failure; CVD, cardiovascular disease; GRC, General Responder Cohort; MI, myocardial infarction; WTCHP, World Trade Center Health Program.
Conditions not mutually exclusive.
Some CVD comorbidity was observed. A considerable percentage diagnosed with CAD also reported heart attacks (15.3%), stroke (5.1%), and CHF (2.8%; Figure 1); few (n = 36, 1.5%) had reported three or more CVD conditions.
FIGURE 1.
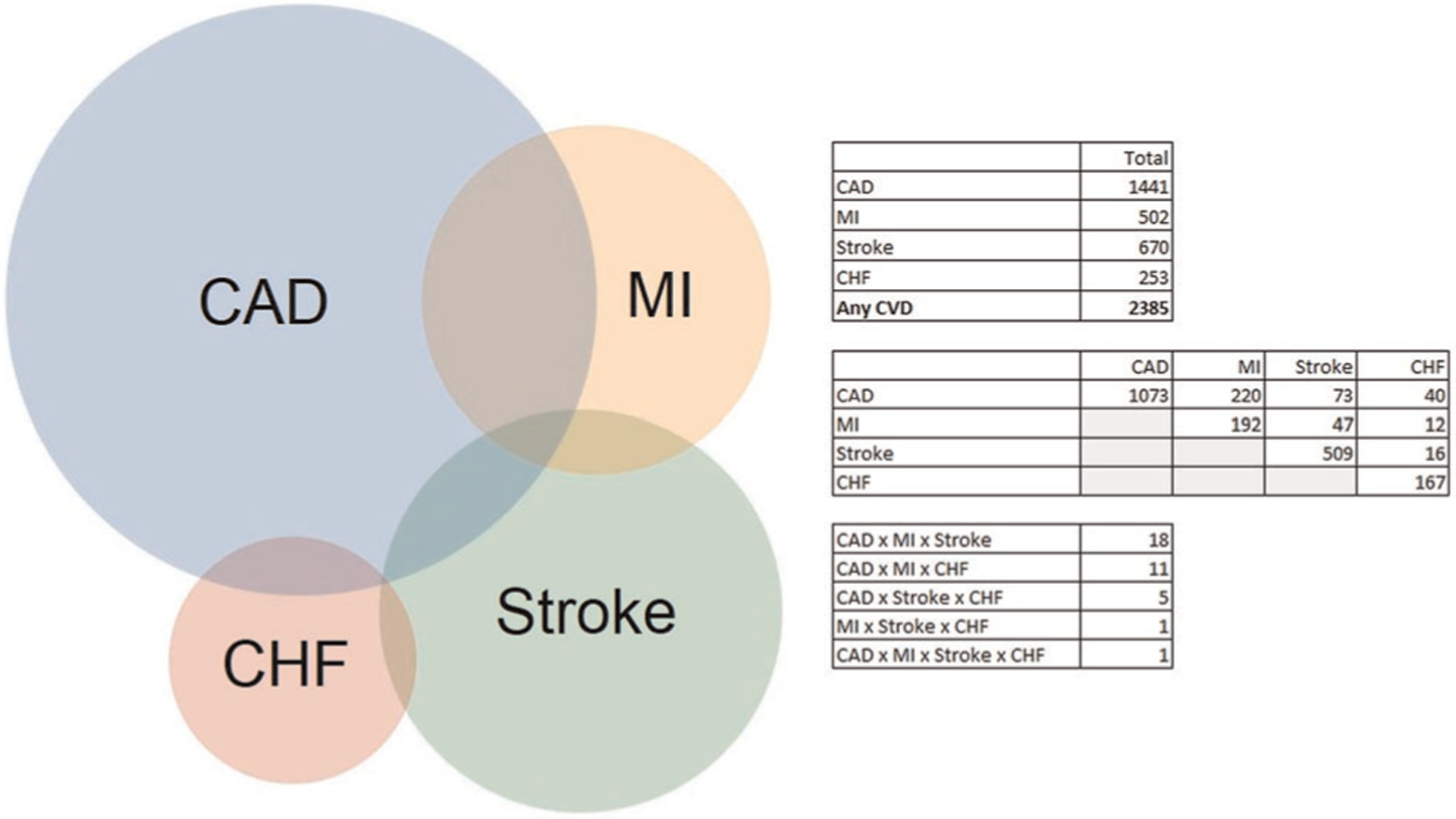
Distribution of post 9/11 CVD (n = 2385) in World Trade Center Health Program General Responder Cohort. CAD, coronary artery disease; CHF, congestive heart failure; CVD, cardiovascular disease; MI, myocardial infarction
Within 5 years of 9/11/2001, the annual CVD incidence increased from <1% in all responders by 0.7% in the general responders who initiated work on or after 9/12, compared with 1.2% among those presenting for work on 9/11/2001 (Table 3, Figures 2 and 3). Eight years after 9/11/2001, the mean time for the cohort’s CVD diagnoses, the annual incidence in those arriving on or after 9/12/2001 had quadrupled to 2.0% compared with 2.5% and 3.1%, among those arriving on 9/11/2001 who were not and who were exposed to the dust cloud, respectively. The cumulative incidence across these exposure groups remained similar until the fourth year after 9/11/2001. By eight years after 9/11/2001, the cumulative CVD incidence was 12.5% among those arriving on 9/11/2001 not exposed to the dust cloud and 13.5% among those exposed to the dust cloud, compared with 9.6% in those arriving on or after 9/12. The CVD incidence patterns were virtually identical among men and women (data not shown).
TABLE 3.
Kaplan–Meier cumulative and annual cardiovascular disease incidence by years since 9/11/2001 (n = 37,725)
| Years since 9/11/2001 | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cumulative incidence (%) | ||||||||||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | |
| ≥9/12 | 0.4 | 0.9 | 1.6 | 2.7 | 3.5 | 4.7 | 5.9 | 7.6 | 9.6 | 11.5 | 13.7 | 15.8 | 18.5 | 22.1 | 25.6 | 30.4 | 36.4 | 43.1 |
| 9/11, not in dust | 0.3 | 0.7 | 1.7 | 3.0 | 4.5 | 6.1 | 8.0 | 10.0 | 12.5 | 14.2 | 16.7 | 19.4 | 22.8 | 28.7 | 34.6 | 43.3 | 49.7 | NA |
| 9/11, in dust cloud | 0.4 | 0.9 | 1.7 | 2.9 | 4.7 | 6.4 | 8.3 | 10.4 | 13.5 | 15.8 | 18.6 | 22.3 | 25.9 | 27.9 | 33.7 | 40.7 | 45.8 | 55.2 |
| Annual incidence (%) | ||||||||||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | |
| ≥9/12 | 0.5 | 0.7 | 1.1 | 0.8 | 1.2 | 1.2 | 1.7 | 2.0 | 1.9 | 2.2 | 2.1 | 2.7 | 3.6 | 3.5 | 4.8 | 6.0 | 6.7 | |
| 9/11, not in dust | 0.4 | 1.0 | 1.3 | 1.5 | 1.6 | 1.9 | 2.0 | 2.5 | 1.7 | 2.5 | 2.7 | 3.4 | 5.9 | 5.9 | 8.7 | 6.4 | NA | |
| 9/11, in dust cloud | 0.5 | 0.8 | 1.2 | 1.8 | 1.7 | 1.9 | 2.1 | 3.1 | 2.3 | 2.8 | 3.7 | 3.6 | 2.0 | 5.8 | 7.0 | 5.1 | 9.4 | |
| Number at risk | ||||||||||||||||||
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | |
| ≥9/12 | 20,865 | 15,032 | 8676 | 7300 | 6392 | 5954 | 5463 | 4924 | 4360 | 3825 | 3287 | 2846 | 2381 | 1823 | 1347 | 994 | 640 | 56 |
| 9/11, not in dust | 9672 | 6725 | 3622 | 2974 | 2584 | 2373 | 2127 | 1904 | 1666 | 1441 | 1257 | 1071 | 883 | 645 | 480 | 316 | 159 | 15 |
| 9/11, in dust cloud | 7185 | 5124 | 2860 | 2309 | 2004 | 1834 | 1642 | 1457 | 1289 | 1100 | 955 | 793 | 661 | 477 | 362 | 263 | 161 | 28 |
FIGURE 2.
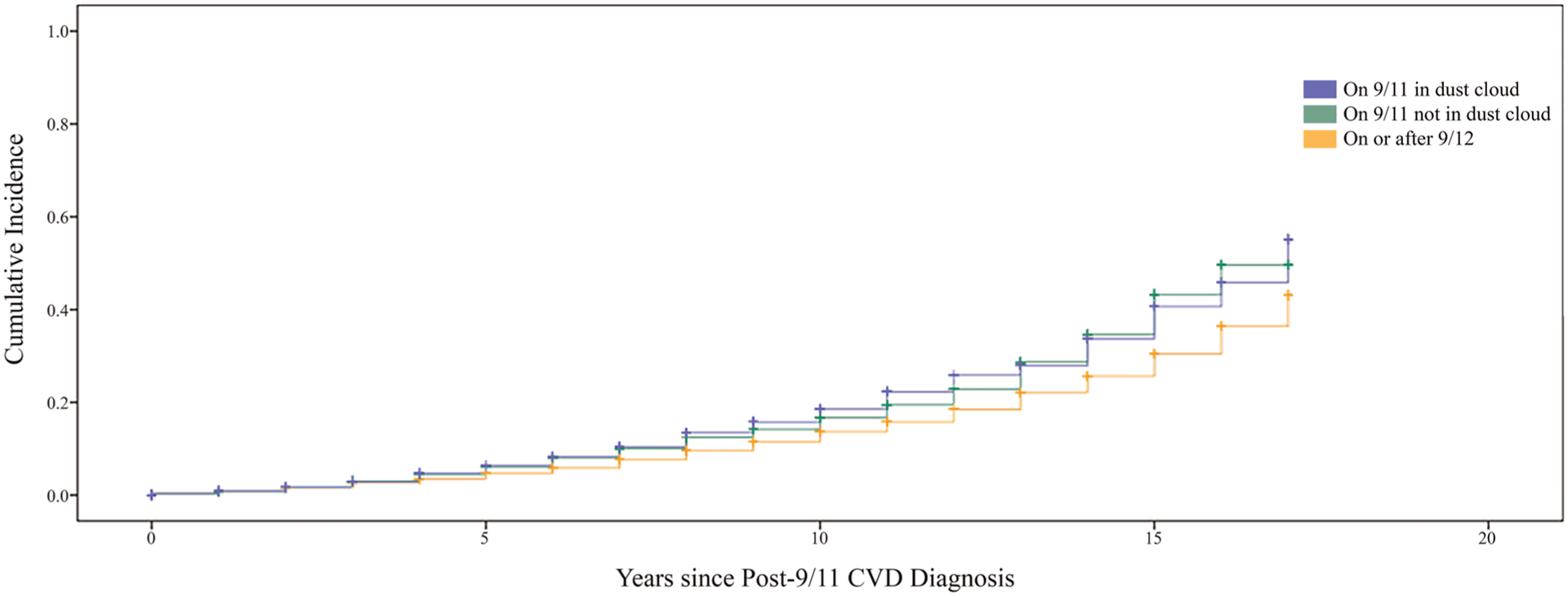
Kaplan–Meier post 9/11 cardiovascular disease (CVD) incidence by years since 9/11/2001
FIGURE 3.
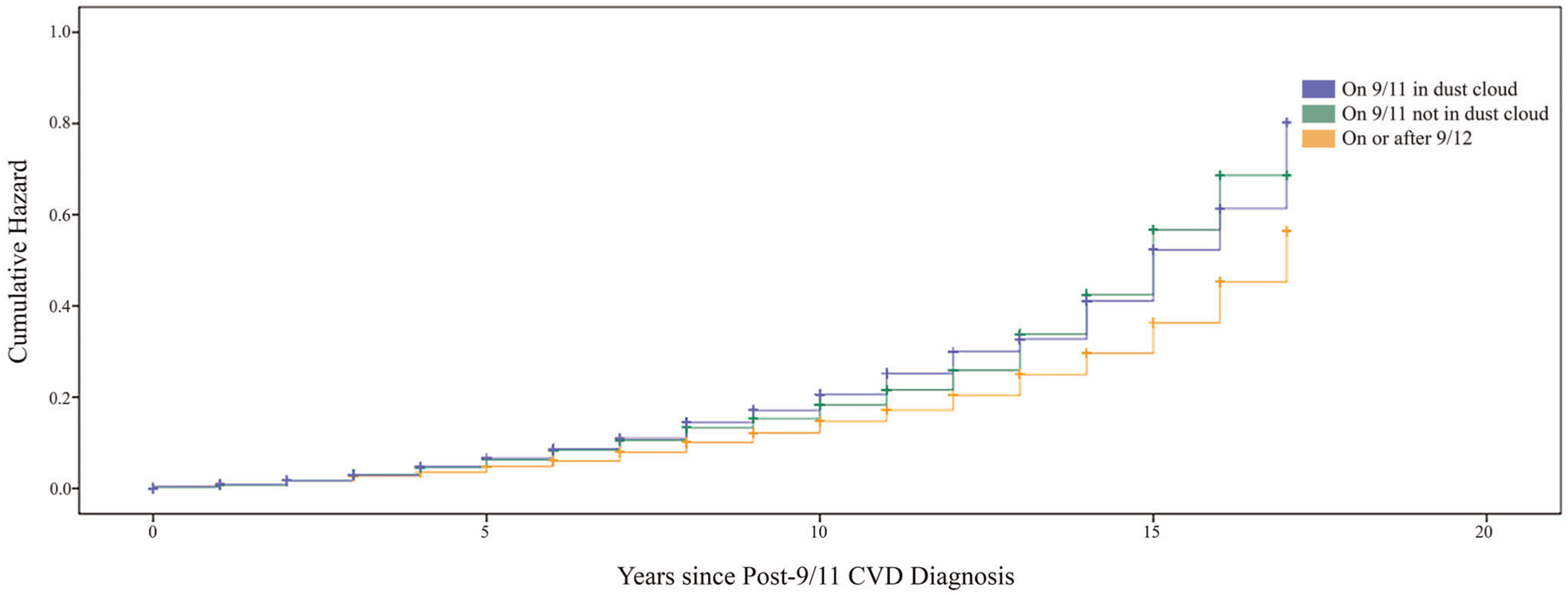
Kaplan–Meier post 9/11 cardiovascular disease (CVD) cumulative hazard by years since 9/11/2001
Men’s covariate-adjusted risk of CVD was substantially higher in 9/11/2001 arrivals not exposed to the dust cloud (HRcov = 1.43; 95% CI = 1.29, 1.58) and in those exposed to the dust cloud (HRcov = 1.40; 95% CI = 1.26, 1.56) than that of general responders arriving on or after 9/12/2001 (Table 4). Additional adjustment for comorbidities reduced men’s overall risk compared with those arriving later to HRcov_comorb = 1.33; 95% CI = 1.20, 1.47 in those without dust cloud exposure and hazard ratio (HR) = 1.29; 95% CI = 1.16, 1.44 in those with dust cloud exposure. There was no substantial violation of the proportional hazards assumptions in the covariate-adjusted model; however, some violation of the assumptions was observed for smoking, cholesterol, and BMI status in the model adjusted for comorbidities. The sensitivity analysis adding log survival time interactions for the violating variables (BMI, smoking, and cholesterol status) produced nearly identical risk estimates as the non-timed dependent model (HRcov_comorb = 1.33; 95% CI = 1.20, 1.47 in those without dust cloud exposure and HRcov_comorb = 1.28; 95% CI = 1.15, 1.43 in those with dust cloud exposure).
TABLE 4.
Cox proportional hazards regression of age to CVD diagnosis
| Men (n = 32,539) | Women (n = 5186) | |||||||
|---|---|---|---|---|---|---|---|---|
| 95% CI | 95% CI | |||||||
| HR | Lower | Upper | p | HR | Lower | Upper | p | |
| Covariate adjusted | ||||||||
| 9/11, not in dust cloud | 1.43 | 1.29 | 1.58 | ≤0.001 | 1.59 | 1.11 | 2.27 | 0.01 |
| 9/11, in dust cloud | 1.40 | 1.26 | 1.56 | ≤0.001 | 2.16 | 1.49 | 3.11 | ≤0.001 |
| White, non-Hispanic | ||||||||
| Black, non-Hispanic | 0.79 | 0.68 | 0.92 | 0.003 | 1.84 | 1.28 | 2.64 | ≤0.001 |
| Asian, non-Hispanic | 1.23 | 0.84 | 1.81 | 0.28 | 0.44 | 0.06 | 3.18 | 0.41 |
| Hispanic | 0.83 | 0.73 | 0.95 | 0.006 | 1.28 | 0.89 | 1.82 | 0.18 |
| Other or not reported | 1.03 | 0.91 | 1.16 | 0.66 | 0.90 | 0.51 | 1.58 | 0.72 |
| Covariate and comorbidity adjusted | ||||||||
| 9/11, not in dust cloud | 1.33 | 1.20 | 1.47 | ≤0.001 | 1.49 | 1.04 | 2.13 | 0.03 |
| 9/11, in dust cloud | 1.29 | 1.16 | 1.44 | ≤0.001 | 2.17 | 1.50 | 3.14 | ≤0.001 |
| White, non-Hispanic | ||||||||
| Black, non-Hispanic | 0.87 | 0.74 | 1.01 | 0.07 | 1.52 | 1.04 | 2.24 | 0.03 |
| Asian, non-Hispanic | 1.13 | 0.77 | 1.67 | 0.53 | 0.62 | 0.08 | 4.54 | 0.64 |
| Hispanic | 0.95 | 0.83 | 1.08 | 0.41 | 1.31 | 0.91 | 1.90 | 0.15 |
| Other or not reported | 1.03 | 0.91 | 1.15 | 0.67 | 0.95 | 0.54 | 1.66 | 0.85 |
| Nonsmoker | ||||||||
| Former smoker | 0.98 | 0.89 | 1.07 | 0.59 | 1.42 | 1.03 | 1.96 | 0.03 |
| Current smoker | 1.55 | 1.33 | 1.80 | ≤0.001 | 1.89 | 1.09 | 3.28 | 0.02 |
| Normal (BMI < 25) | ||||||||
| Overweight (BMI, 25–29) | 1.25 | 1.07 | 1.47 | 0.005 | 1.04 | 0.71 | 1.51 | 0.86 |
| Obese (BMI ≥ 30) | 1.56 | 1.34 | 1.83 | ≤0.001 | 1.31 | 0.89 | 1.92 | 0.17 |
| Ever had diabetes | 1.21 | 1.10 | 1.33 | ≤0.001 | 1.52 | 1.07 | 2.16 | 0.02 |
| Ever had high blood pressure | 1.46 | 1.31 | 1.63 | ≤0.001 | 1.28 | 0.92 | 1.78 | 0.14 |
| Ever had high cholesterol | 5.61 | 4.92 | 6.39 | ≤0.001 | 2.76 | 1.93 | 3.94 | ≤0.001 |
Abbreviations: BMI, body mass index; CI, confidence interval; CVD, cardiovascular disease; HR, hazard ratio.
Women’s covariate-adjusted risks were HRcov_comorb = 1.59; 95% CI = 1.11, 2.27 in responders arriving on 9/11/2001 without dust cloud exposure and HRcov_comorb = 2.16; 95% CI = 1.39, 3.11 in responders arriving on 9/11/2001 with dust cloud exposure, compared with women arriving on or after 9/12. When adjusted for comorbidities, women arriving on 9/11/2001 without dust cloud exposure had HRcov_comorb = 1.49; 95% CI = 1.04, 2.13 and HRcov_comorb = 2.17; 95% CI = 1.34, 3.14 with dust cloud exposure compared with women arriving on or after 9/12/2001. No violation of the proportional hazards assumptions was observed in the women’s analyses.
Except for Hispanic men who had lower CVD risk than white non-Hispanic responders in the covariate-adjusted model, the hazards ratios for race/ethnicity all had 95% CIs that included the null value of 1. Current cigarette smokers had higher CVD risk in men and women, but former smokers only had higher CVD risk in women than lifetime nonsmokers. Overweight and obesity at a responder’s first visit was associated with CVD risk but only significantly so in men. Responders who had ever been diagnosed with diabetes, high blood pressure, and/or high cholesterol had significantly higher CVD risk than those never diagnosed with those conditions, except in women with high blood pressure. The associations with smoking, cholesterol, and BMI status should not be over-interpreted as violations of the proportional hazards assumptions were observed for these indices. In additional multivariate analyses (data not shown), having been diagnosed with cancer before CVD was highly associated with CVD.
WTCHP GRC protective services occupational status on 9/11/2001 was significantly different among those arriving on or after 9/12/2001 than those responding on 9/11/2001. Over 65% of men and 71% of women 9/11 arrivals (in those exposed and not exposed to the dust cloud) were engaged in protective services employment on 9/11. Only 42% of men and 44% of women arriving on or after 9/12 were engaged in protective services on 9/11. Therefore, sensitivity analyses adjusting for protective services occupation on 9/11 were conducted. Compared with all other responders, active occupation in protective services on 9/11/2001 was associated with increased risk of CVD in men (HRcov = 2.07; 95% CI = 1.89, 2.27) and women (HRcov = 2.81; 95% CI = 2.02, 3.90; Table 5). Higher protective services HRs were observed in the comorbidity-adjusted models. Adjustment for 9/11/2001 protective services occupational status reduced the CVD risks associated with 9/11/2001 arrival, particularly in the comorbidity-adjusted analysis of men reporting dust cloud exposure and in both the covariate and covariate/comorbidity-adjusted analysis of women not reporting dust cloud exposure, to risks with confidence limits crossing the null value of 1. Sensitivity analyses adding log survival time interactions for the violating covariates and comorbidities produced similar results. Analyses of the total sample (both sexes) combining arrivals on 9/11 with and without dust cloud exposure that were adjusted for 9/11 protective services occupation had a 9/11 arrival HRcov = 1.21; 95% CI = 1.12, 1.32 in the covariate-adjusted model and HRcov_comorb = 1.12; 95% CI = 1.03, 1.22 (with no violations for the primary factor of interest).
TABLE 5.
Cox proportional hazards regression of age to CVD diagnosis including protective services occupation on 9/11/2001
| Men (n = 32,539) | Women (n = 5186) | |||||||
|---|---|---|---|---|---|---|---|---|
| 95% CI | 95% CI | |||||||
| HR | Lower | Upper | p | HR | Lower | Upper | p | |
| Covariate adjusted | ||||||||
| 9/11, not in dust cloud | 1.24 | 1.12 | 1.38 | ≤0.001 | 1.25 | 0.87 | 1.80 | 0.23 |
| 9/11, in dust cloud | 1.14 | 1.02 | 1.28 | 0.02 | 1.71 | 1.17 | 2.48 | 0.005 |
| White, non-Hispanic | ||||||||
| Black, non-Hispanic | 0.83 | 0.71 | 0.97 | 0.02 | 1.49 | 1.03 | 2.16 | 0.04 |
| Asian, non-Hispanic | 1.31 | 0.89 | 1.91 | 0.17 | 0.34 | 0.05 | 2.47 | 0.29 |
| Hispanic | 0.86 | 0.75 | 0.98 | 0.02 | 1.25 | 0.88 | 1.78 | 0.21 |
| Other or not reported | 1.04 | 0.92 | 1.17 | 0.53 | 0.81 | 0.46 | 1.42 | 0.47 |
| Protective services | 2.07 | 1.89 | 2.27 | ≤0.001 | 2.81 | 2.02 | 3.90 | ≤0.001 |
| Covariate and comorbidity adjusted | ||||||||
| 9/11, not in dust cloud | 1.16 | 1.05 | 1.28 | 0.005 | 1.18 | 0.82 | 1.70 | 0.38 |
| 9/11, in dust cloud | 1.04 | 0.93 | 1.17 | 0.46 | 1.61 | 1.10 | 2.36 | 0.02 |
| White, non-Hispanic | ||||||||
| Black, non-Hispanic | 0.91 | 0.78 | 1.06 | 0.22 | 1.20 | 0.81 | 1.78 | 0.37 |
| Asian, non-Hispanic | 1.16 | 0.79 | 1.71 | 0.44 | 0.42 | 0.06 | 3.14 | 0.40 |
| Hispanic | 0.97 | 0.85 | 1.11 | 0.66 | 1.28 | 0.89 | 1.85 | 0.19 |
| Other or not reported | 1.00 | 0.89 | 1.13 | 0.97 | 0.83 | 0.47 | 1.47 | 0.53 |
| Nonsmoker | ||||||||
| Former smoker | 1.02 | 0.93 | 1.12 | 0.62 | 1.33 | 0.97 | 1.84 | 0.08 |
| Current smoker | 1.77 | 1.52 | 2.06 | ≤0.001 | 1.67 | 0.96 | 2.91 | 0.07 |
| Normal (BMI < 25) | ||||||||
| Overweight (BMI, 25–29) | 1.20 | 1.02 | 1.41 | 0.03 | 0.96 | 0.66 | 1.41 | 0.84 |
| Obese (BMI ≥ 30) | 1.46 | 1.25 | 1.71 | ≤0.001 | 1.19 | 0.81 | 1.75 | 0.38 |
| Ever had diabetes | 1.25 | 1.14 | 1.38 | ≤0.001 | 1.44 | 1.01 | 2.06 | 0.04 |
| Ever had high blood pressure | 1.48 | 1.33 | 1.65 | ≤0.001 | 1.33 | 0.96 | 1.85 | 0.09 |
| Ever had high cholesterol | 5.50 | 4.83 | 6.27 | ≤0.001 | 2.90 | 2.03 | 4.15 | ≤0.001 |
| Protective services | 2.16 | 1.97 | 2.37 | ≤0.001 | 2.94 | 2.10 | 4.11 | ≤0.001 |
Abbreviations: BMI, body mass index; CI, confidence interval; CVD, cardiovascular disease; HR, hazard ratio.
Because those enrolling later in the health monitoring program had fewer visits, we assessed whether age at diagnosis varied by enrollment period. Men who enrolled in the first 5 years of the monitoring program (50% of men’s CVD cases) reported they were 53 ± 9 years old at their first CVD diagnosis, as did the men who enrolled in the last 4 years of the program (26% of men’s CVD cases). Men who enrolled between 2008 and 2013 reported being a year and a half younger (±9 years) at their first CVD diagnosis. Women who enrolled in the first 5 years (before 2007, 58% of women’s cases) and the following 5 years (2008–2013, 25% of women’s cases) reported being 51 ± 10 years old at their first CVD diagnosis, whereas the 17% (n = 33) enrolled in the last 4 years reported they were 56 ± 13 years old at their first diagnosis of CVD.
4 |. DISCUSSION
Globally, heart disease remains the leading cause of death.1–3 In some studies, exposure to air pollution, radioactive materials, environmental toxic metals, and other particulate matter identified in the WTC disaster have been associated with increased risk of cardiac dysfunction, heart disease, and death. With 17 years’ follow-up of a large cohort of WTC general responders, we observed substantially higher risks of CVD associated with initiating work on 9/11/2001 compared with responders who initiated work on or after 9/12.
This study found 9/11/2001 arrival was associated with elevated CVD risk in men and women compared with responders arriving on or after 9/12. Despite the somewhat different definitions of CVD used in our and in the FDNY analyses, the analysis of men’s risk adjusted for nearly identical covariates and comorbidities demonstrate WTC 9/11 exposures are associated with large, statistically significant increased hazards for CVD, consistent with observations in the all-male sample of firefighter responders.30 This consistency with the male FDNY results is notable, as their criteria for CVD was based upon the theoretically more accurate (than a responder’s recall, particularly regarding event dates) physicians’ diagnosis from electronic medical records.30 Except for women presenting on 9/11/2001 without dust cloud exposure, the WTCHP GRC lower 95% CIs were all well above 1. The association with dust cloud exposure was less clear among men, who comprise the vast majority of the sample, whereas a clear elevated CVD risk was observed with arrival on 9/11 in the total sample.
Distinct from the FDNY responders, the WTCHP GRC includes a substantial female cohort. With its large sample of female general responders, the WTCHP GRC also identified large risk differences associated with 9/11/2001 compared with later exposure among female responders, even though there was a 45% lower post 9/11/2001 CVD prevalence among female than male responders. The risk in women associated with 9/11/2001 exposure was much greater than the elevated men’s 9/11/2001 CVD risk compared with those presenting on or after 9/12/2001. This may indicate that the female general responders have less chronic or previous hazardous environmental exposures and, therefore, have a greater reaction to the toxic 9/11/2001 exposures than do men. Alternatively, because the cohort of female general responders is so much smaller than that of men, they may simply represent a less diverse group of responders than men. Women’s hazards ratios had wider 95% CIs than that of men’s, reflecting the smaller sample size for female responders.
Over half of the WTCHP GRC were employed in protective services (high-stress occupations) which, among other occupations (such as transportation and moving materials) have been identified as CVD risk factors.34,35 Employment in protective services was associated with CVD, and specifically attenuated the risks of men with dust cloud exposure risks to the extent that their confidence limits crossed the value of 1 (no effect). Conversely, adjustment for 9/11 occupation in protective services obviated the excess CVD risk in women without dust cloud exposure. These observations suggest that the risks associated with protective services employment share common characteristics with 9/11 arrival, although there was no significant interaction between arrival time and 9/11 protective services occupation (data not shown). Still, when all 9/11 arrivals for the total sample (both sexes, whether exposed to the dust cloud or not) were combined, adjustment for being engaged in protective services on 9/11 reduced but did not nullify the excess CVD risk in the WTCHP GRC.
Known risk factors for CVD include age, poor diet, cigarette smoking, high blood pressure, high cholesterol, diabetes, and work psychosocial stressors.2,3,5–7,23,34,35 Analyses adjusted and stratified for these risk factors were conducted. Consistent with the literature,1–3 being Hispanic was associated with lower men’s CVD risk in the covariate-adjusted analyses, but not in the remaining analyses where the confidence limits for race/ethnicity risk crossed the null value of 1. The associations of measured BMI at the first health monitoring visit and smoking were generally in the expected direction. Although the observed associations with the participants’ reports of ever being diagnosed with high blood pressure, high cholesterol, and diabetes were in the expected direction, they are flawed in this evaluation because dates of their initial diagnoses were often missing, offering no assurance that these conditions occurred before the self-reported CVD diagnosis. As violations of the proportional hazards assumptions were observed for smoking, cholesterol, and BMI status, their associations with CVD risk in this study should not be over-interpreted. Adjustment for comorbidities and risk factors, including smoking, overweight and obesity, hypertension, diabetes, and high cholesterol, all of which may be partially caused or exacerbated by the 9/11/2001 exposures, and are in the causal pathway for CVD, may overcontrol and underestimate the 9/11 exposure effects.
The WTCHP GRC CVD risk may also be occurring much earlier than observed in the general population. The WTCHP GRC’s average age at heart attack was 52 years old compared with the US general population with an average age at heart attack of 64 in men and 70 in women.2,3,5,6,37 In the WTCHP GRC, only 4% of CVD occurred at or after age 65. Among the WTCHP GRC, 16% of men’s heart attacks occurred before age 45 compared with 4%–10% of men’s heart attacks in the general population.38
This investigation used robust statistical methods to assess the association of WTCHP GRC environmental exposure and CVD risk among a large cohort of men and women. Categorizing those with a reported heart murmur and other heart diseases as noncases may have attenuated the observed results. Similarly, if responders, particularly those engaged in physically demanding work, are relatively healthy and thus at lower risk for adverse health outcomes, this healthy worker effect may have biased our observed effects of 9/11 exposure toward the null. The results also depend upon the accuracy of participant reports of diagnosis and/or treatment for CVD, in this study. The CVD conditions assessed in this study are major life events. Regardless, the validity of self-reported CVD is imperfect. Correct case identification of MI has been found to be better (ranging from 50% to 98%) than stoke (ranging from 38% to 81%) in various populations.39–41 While overreporting is more common than underreporting, bidirectional misreporting has been observed. The lack of lifetime primary care medical records, against which to validate the health monitoring program’s self-reported CVD diagnoses, is a study limitation. The consistency of men’s elevated CVD risk with that of the FDNY suggests that the men’s self-reported physician’s diagnosis of CVD was not unduly influenced by recall bias. Relatively few women reporting CVD enrolled in the last 4 years of the monitoring program, and the influence of any women’s recall bias may be limited. The results are consistent with the extant literature in both the direction and magnitude of 9/11/2001 exposure effects and its higher risk of heart disease.27–30 While the FDNY data were limited to male responders, Jordan et al. also found an increased risk of heart disease in female responders with intense dust cloud exposure compared with less exposed women.28,30,42
As a voluntary program, the extent to which WTCHP GRC participants represent all WTC first responders is unknown. Compared with the FDNY program, the WTCHP GRC provides services to and obtains information on a more diverse group of general responders. While continuing to enroll responders, the WTCHP GRC has experienced diminishing numbers of responders presenting for monitoring visits over time. The considerable decline in and the possible self-selection of responders presenting for HP monitoring visits among those who are symptomatic or ill potentially explains the increasingly high cumulative incidence over time.
In summary, this evaluation observed a substantially higher risk of CVD associated with WTCHP GRC members initiating work on 9/11/2001 compared with those who initiated work on or after 9/12, with women’s risk greater than that of men’s. Elevated CVD risk may also be occurring at a younger age in responders than in the general population. Active engagement in protective services on 9/11/2001 is associated with increased CVD risk. The study findings reinforce the need for broadening public awareness about the associations of WTC exposure and CVD and for continued monitoring of the WTCHP GRC to identify and treat heart disease and promote CVD prevention (e.g., through diet, exercise, weight control, smoking cessation, work stressor reduction, etc.) as a means to minimize its life-altering and life-threatening consequences.
ACKNOWLEDGMENTS
We thank the WTCHP and Data Center staff, the labor, community, and volunteer organization stakeholders; and the WTC GRC who so readily and generously gave of themselves in response to the WTC terrorist attacks and to whom the WTC programs are dedicated. This study was supported by grant sponsor Centers for Disease Control and Prevention/National Institute for Occupational Safety and Health; through cooperative agreements and contracts 200-2002-00384, U10-OH008216/23/25/32/39/75, 200-2011-39356/61/77/84/85/88, and 200-2017-93325.
Footnotes
CONFLICTS OF INTEREST
The authors declare that there are no conflicts of interest.
DISCLOSURE BY AJIM EDITOR OF RECORD
Paul A. Landsbergis declares that he has no conflict of interest in the review and publication decision regarding this article.
DATA AVAILABILITY STATEMENT
The relevant data are available within the manuscript. The access to the study’s de-identified data and analytic code requires IRB approval, and submission and approval of the WTC Data Center Data Use Agreement, and Data Request Form (including an attestation), which may be requested of the corresponding author.
ETHICS APPROVAL AND INFORMED CONSENT
This study has been conducted in accordance with the principles of the Declaration of Helsinki 1975, as revised in 2013, and complies with the ethical standards of the relevant national and institutional committees on human experimentation. The work was performed and the WTCHP research has been approved by the Institutional Review Boards (IRBs) of the Icahn School of Medicine at Mount Sinai (formerly Mount Sinai School of Medicine), New York, NY and the program’s other clinical sites, including New York University Langone Medical Center, New York University School of Medicine, New York, NY; Department of Medicine, Stony Brook University Medical Center, Stony Brook, NY; Department of Occupational Medicine, Epidemiology and Prevention, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY; and Environmental and Occupational Health Sciences Institute, Rutgers University, Piscataway, NJ.
Publisher's Disclaimer: DISCLAIMER
Publisher's Disclaimer: The contents of this report are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or the National Institute for Occupational Safety and Health.
REFERENCES
- 1.Benjamin EJ, Muntner P, Alonso A, et al. Heart Disease and Stroke Statistics-2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56–e528. [DOI] [PubMed] [Google Scholar]
- 2.Heron M. Leading Causes of Death for 2017 Washington, DC: National Center for Health Statistics; 2019. https://www.cdc.gov/nchs/data/nvsr/nvsr68/nvsr68_06-508.pdf. Accessed September 5, 2019. [Google Scholar]
- 3.Nowbar AN, Gitto M, Howard JP, Francis DP, Al-Lamee R. Mortality from ischemic heart disease. Circ Cardiovasc Qual Outcomes. 2019; 12(6):e005375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dagenais GR, Leong DP, Rangarajan S, et al. Variations in common diseases, hospital admissions, and deaths in middle-aged adults in 21 countries from five continents (PURE): a prospective cohort study. Lancet. 2019;395:785–794. [DOI] [PubMed] [Google Scholar]
- 5.Dawber TR, Meadors GF, Moore FE Jr. Epidemiological approaches to heart disease: the Framingham Study. Am J Public Health Nations Health. 1951;41(3):279–281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mahmood SS, Levy D, Vasan RS, Wang TJ. The Framingham Heart Study and the epidemiology of cardiovascular disease: a historical perspective. Lancet. 2014;383(9921):999–1008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Backe EM, Seidler A, Latza U, Rossnagel K, Schumann B. The role of psychosocial stress at work for the development of cardiovascular diseases: a systematic review. Int Arch Occup Environ Health. 2012; 85(1):67–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Brook RD, Rajagopalan S, Pope CA 3rd, et al. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation. 2010; 121(21):2331–2378. [DOI] [PubMed] [Google Scholar]
- 9.Chowdhury R, Ramond A, O’Keeffe LM, et al. Environmental toxic metal contaminants and risk of cardiovascular disease: systematic review and meta-analysis. BMJ. 2018;362:k3310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Miller KA, Siscovick DS, Sheppard L, et al. Long-term exposure to air pollution and incidence of cardiovascular events in women. N Engl J Med. 2007;356(5):447–458. [DOI] [PubMed] [Google Scholar]
- 11.Pope CA 3rd, Dockery DW. Health effects of fine particulate air pollution: lines that connect. J Air Waste Manag Assoc. 2006;56(6): 709–742. [DOI] [PubMed] [Google Scholar]
- 12.World Health Organization. Air Quality Guidelines Global Update 2005: Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide. Germany: WHO Regional Office for Europe; 2006. http://www.euro.who.int/__data/assets/pdf_file/0005/78638/E90038.pdf [Google Scholar]
- 13.Yang BY, Guo Y, Morawska L, et al. Ambient PM1 air pollution and cardiovascular disease prevalence: insights from the 33 Communities Chinese Health Study. Environ Int. 2019;123:310–317. [DOI] [PubMed] [Google Scholar]
- 14.Zhang Z, Guo C, Lau AKH, et al. Long-term exposure to fine particulate matter, blood pressure, and incident hypertension in Taiwanese adults. Environ Health Perspect. 2018;126(1):017008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gellissen J, Pattloch D, Mohner M. Effects of occupational exposure to respirable quartz dust on acute myocardial infarction. Occup Environ Med. 2019;76(6):370–375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ljungman PLS, Li W, Rice MB, et al. Long- and short-term air pollution exposure and measures of arterial stiffness in the Framingham Heart Study. Environ Int. 2018;121(Pt 1):139–147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sjogren B. Occupational exposure to dust: inflammation and ischaemic heart disease. Occup Environ Med. 1997;54(7): 466–469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Boffetta P, Zeig-Owens R, Wallenstein S, et al. Cancer in World Trade Center responders: findings from multiple cohorts and options for future study. Am J Ind Med. 2016;59(2):96–105. [DOI] [PubMed] [Google Scholar]
- 19.New York City 9/11 Health. Rescue and Recovery Workers: Search City of New York; 2019. https://www1.nyc.gov/site/911health/enrollees/rescue-recovery-workers.page. Accessed December 16, 2019.
- 20.Savitz DA, Oxman RT, Metzger KB, et al. Epidemiologic research on man-made disasters: strategies and implications of cohort definition for World Trade Center worker and volunteer surveillance program. Mt Sinai J Med. 2008;75(2):77–87. [DOI] [PubMed] [Google Scholar]
- 21.Lioy PJ, Weisel CP, Millette JR, et al. Characterization of the dust/smoke aerosol that settled east of the World Trade Center (WTC) in lower Manhattan after the collapse of the WTC 11 September 2001. Environ Health Perspect. 2002;110(7):703–714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Howard J. World Trade Center Health Program Development of the Inventory of 9/11 Agents ResearchGateway: World Trade Center Health Program; 2018. https://wwwn.cdc.gov/ResearchGateway/Content/pdfs/Development_of_the_Inventory_of_9-11_Agents_20180717.pdf. Accessed September 5, 2019.
- 23.Schnall PL, Dobson M, Landsbergis P. Globalization, work, and cardiovascular disease. Int J Health Serv. 2016;46(4):656–692. [DOI] [PubMed] [Google Scholar]
- 24.Herbert R, Moline J, Skloot G, et al. The World Trade Center disaster and the health of workers: five-year assessment of a unique medical screening program. Environ Health Perspect. 2006;114(12):1853–1858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Landrigan PJ, Lioy PJ, Thurston G, et al. Health and environmental consequences of the World Trade Center disaster. Environ Health Perspect. 2004;112(6):731–739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wisnivesky JP, Teitelbaum SL, Todd AC, et al. Persistence of multiple illnesses in World Trade Center rescue and recovery workers: a cohort study. Lancet. 2011;378(9794):888–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Jordan HT, Brackbill RM, Cone JE, et al. Mortality among survivors of the Sept 11, 2001, World Trade Center disaster: results from the World Trade Center Health Registry cohort. Lancet. 2011;378(9794):879–887. [DOI] [PubMed] [Google Scholar]
- 28.Jordan HT, Stein CR, Li J, et al. Mortality among rescue and recovery workers and community members exposed to the September 11, 2001 World Trade Center terrorist attacks, 2003–2014. Environ Res. 2018;163:270–279. [DOI] [PubMed] [Google Scholar]
- 29.Remch M, Laskaris Z, Flory J, Mora-McLaughlin C, Morabia A. Post-traumatic stress disorder and cardiovascular diseases: a cohort study of men and women involved in cleaning the debris of the World Trade Center complex. Circ Cardiovasc Qual Outcomes. 2018; 11(7):e004572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cohen HW, Zeig-Owens R, Joe C, et al. Long-term cardiovascular disease risk among firefighters after the World Trade Center disaster. JAMA Netw Open. 2019;2(9):e199775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Dasaro CR, Holden WL, Berman KD, et al. Cohort profile: World Trade Center Health Program General Responder Cohort. Int J Epidemiol. 2017;46(2):e9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Moline JM, Herbert R, Levin S, et al. WTC medical monitoring and treatment program: comprehensive health care response in after-math of disaster. Mt Sinai J Med. 2008;75(2):67–75. [DOI] [PubMed] [Google Scholar]
- 33.Caldwell DM, Welton NJ, Dias S, Ades AE. Selecting the best scale for measuring treatment effect in a network meta-analysis: a case study in childhood nocturnal enuresis. Res Synth Methods. 2012;3(2):126–141. [DOI] [PubMed] [Google Scholar]
- 34.Moline JM, McLaughlin MA, Sawit ST, et al. The prevalence of metabolic syndrome among law enforcement officers who responded to the 9/11 World Trade Center attacks. Am J Ind Med. 2016;59(9):752–760. [DOI] [PubMed] [Google Scholar]
- 35.Shockey TM,SA, Odom EC. Cardiovascular Health Status by Occupational Group—21 States, 2013. Centers for Disease Control and Prevention. 2016;65:793–798. [DOI] [PubMed] [Google Scholar]
- 36.Chang HM, Okwuosa TM, Scarabelli T, Moudgil R, Yeh ETH. Cardiovascular complications of cancer therapy: best practices in diagnosis, prevention, and management: part 2. J Am Coll Cardiol. 2017;70(20):2552–2565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Memorial Hermann Heart & Vascular Institute. Heart Disease and Age: Memorial Hermann; 2019. http://heart.memorialhermann.org/education-prevention/heart-disease-and-age/. Accessed October 7, 2019.
- 38.Harvard Medical School. Premature Heart Disease, Cambridge. MA: Harvard Health Publishing; 2009. https://www.health.harvard.edu/heart-health/premature-heart-disease [Google Scholar]
- 39.Smith B, Chu LK, Smith TC, et al. Challenges of self-reported medical conditions and electronic medical records among members of a large military cohort. BMC Med Res Methodol. 2008;8:37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Machón M, Arriola L, Larrañaga N, et al. Validity of self-reported prevalent cases of stroke and acute myocardial infarction in the Spanish cohort of the EPIC study. J Epidemiol Community Health. 2013;67(1):71–75. [DOI] [PubMed] [Google Scholar]
- 41.Barr EL, Tonkin AM, Welborn TA, Shaw JE. Validity of self-reported cardiovascular disease events in comparison to medical record adjudication and a statewide hospital morbidity database: the AusDiab study. Intern Med J. 2009;39(1):49–53. [DOI] [PubMed] [Google Scholar]
- 42.Jordan HT, Miller-Archie SA, Cone JE, Morabia A, Stellman SD. Heart disease among adults exposed to the September 11, 2001 World Trade Center disaster: results from the World Trade Center Health Registry. Prev Med. 2011;53(6):370–376. [DOI] [PubMed] [Google Scholar]