
Figure 6.
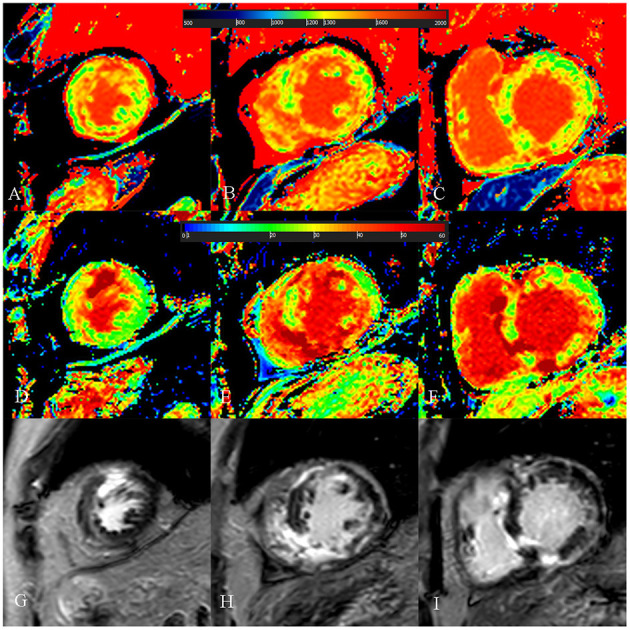
A 52-year-old male with burned out phase hypertrophic cardiomyopathy. (A–C) Native T1 mapping of the apical, mid-, and basal portions of the left ventricular (LV) myocardium revealed higher global native T1 (1,380.7 ms). (D–F) Extracellular volume fraction (ECV) of the apical, mid-, and basal portions of the LV myocardium showed higher global ECV (32.8%). (G–I) Late gadolinium enhancement (LGE) images of the apical, mid-, and basal portions of the LV myocardium showed multiple LGE. The maximal LV wall thickness was 13 mm, left atrial diameter was 53 mm, and the LV outflow tract gradient pressure was 2 mmHg. He had non-sustained ventricular tachycardia, but no family history of sudden cardiac death (SCD), and unexplained syncope. He had LGE/LV mass ≥15% (elevated LGE/LV mass: 56.2%) and end-stage systolic dysfunction but no apical aneurysm. He was stratified with low SCD risk under the 2014 European Society of Cardiology guidelines (5-year SCD probability: 3.39%) and high SCD risk under the enhanced American College of Cardiology/American Heart Association guidelines. He underwent cardiac transplantation 35 months after cardiac MRI examination. End-stage systolic dysfunction strongly indicated poor outcome in this patient. However, increased global native T1 mapping and ECV values could also suggest that the patient was likely to be at high risk of SCD and needs further treatment.