
Figure 1. A spectrum of clinical imaging findings of ATRT.
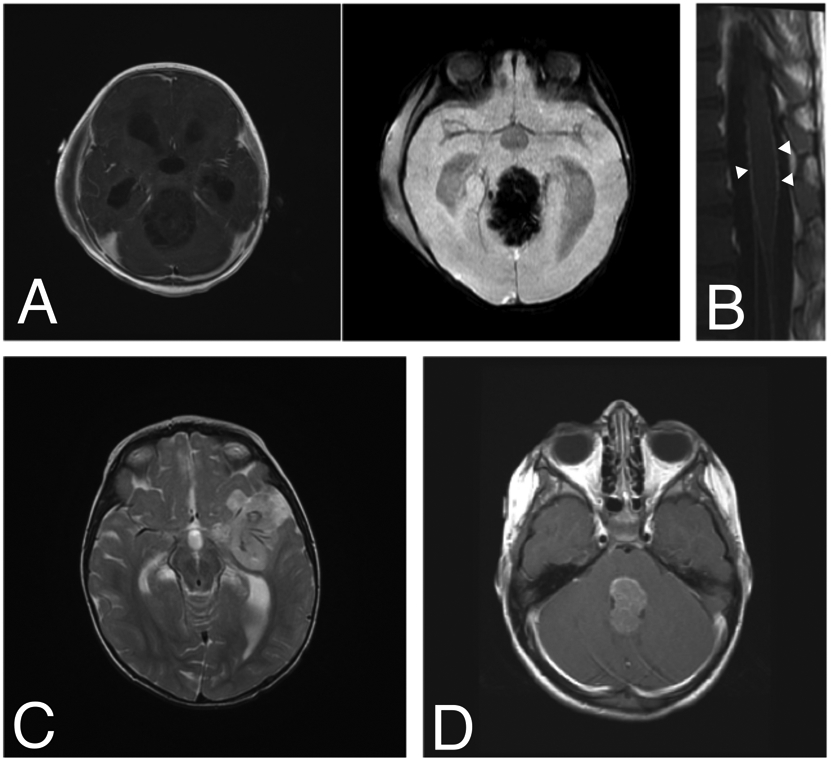
ATRT should be considered in any young child with imaging features of a highly aggressive brain tumor. A) A 9-month-old boy presented with vomiting followed quickly by coma. MRI demonstrated a 6-cm pineal-region mass with minimal, heterogeneous enhancement and abundant vascularity on susceptibility-weighted imaging. B) Diffuse leptomeningeal enhancement of the spinal cord and cauda equina were noted at the time of diagnosis (arrowheads). He underwent a gross total resection (GTR) via suboccipital craniotomy followed by ACNS0333 chemotherapy, stem cell rescue and proton beam radiotherapy with adjuvant craniospinal radiation (CSI). He currently has no evidence of disease three and a half years after diagnosis. C) A 13-month-old girl presented with coma and was found to have a 4-cm left frontotemporal, minimally enhancing mass encasing several large feeding blood vessels (T2-weighted image with contrast shown). She underwent GTR followed by adjuvant chemotherapy using the ACNS0333 protocol, stem-cell transplant and CSI. She is currently seven years since diagnosis and remains disease-free. D) A 4-year-old girl presented with nausea, vomiting and lethargy. MRI demonstrated a 3-cm, homogeneously enhancing fourth ventricular mass (T1-weighted image with contrast shown). She underwent near-total resection via suboccipital craniotomy, adjuvant chemotherapy with the SJMB-06 protocol and CSI. She is free of disease six years post-operatively.