

Keywords: external anal sphincter, fecal incontinence, Kegel exercises
Abstract
Exercises involving pelvic floor muscles including repetitive voluntary contractions of external anal sphincter (EAS) musculature have been used to improve fecal incontinence. Muscle fatigue is a prerequisite for successful strength training. However, muscle fatigue induced by these exercises has not been systematically studied. We aimed to assess the fatigability of EAS muscles during various exercise methods. Twelve nulliparous (21 ± 2.7 yr) women were studied. We evaluated fatigue during 40 repetitive 3-s contractions and 30-s long squeeze contractions both with and without an intra-anal compressible resistant load. The sequence of exercises was randomized. This load was provided by the continence muscles Resistance Exerciser Device. Anal canal pressures were recorded by high-resolution manometry. Exercise against a resistive load showed significant decrease in anal contractile integral (CI) and maximum squeeze pressure during repetitive short squeeze contractions compared with exercise without a load. Linear regression analysis showed a significant negative correlation between anal CI and successive contraction against load, suggesting “fatigue.” Similar findings were observed for maximum squeeze pressure (slope with load = −4.2, P = 0.0003, vs. without load = −0.9, P = 0.3). Long squeeze contraction against a load was also more susceptible to fatigue than without a load (P < 0.0001). In conclusion, repetitive contractions against a compressible load induce fatigue and thus have the potential to strengthen the anal sphincter contractile function than contractions without a load. Fatigue rate in long squeeze contraction exercises with a load is significantly faster than that without a load, also indicating greater effectiveness in inducing muscle fatigue.
NEW & NOTEWORTHY Fecal incontinence is a distressing disorder with a mainstay of treatment being pelvic floor muscle exercises. However, none of these exercises has proven occurrence of fatigability, which is an important prerequisite for successful muscle strengthening in rehabilitative exercises. In this study, we proved that we can fatigue the external anal sphincter muscles more efficiently by providing a resistive load during anal repetitive short squeeze contractions and long squeeze contraction exercise.
INTRODUCTION
Fecal incontinence (FI) is a distressing and socially debilitating disorder that constitutes a major health problem worldwide with a prevalence ranging from 7% to 15% (1, 2). There is a similar prevalence of FI in men and women reported by some studies (3, 4). Individuals who are suffering from FI are unable to control the time and location of bowel movements, leading to involuntary loss of solid or liquid feces. Incontinence can result in secondary comorbidities such as skin maceration, urinary tract infections, and decubitus ulcers (5). FI has a significant impact on quality of life for the patients and caregivers (1, 6–8).
Continence is a complex process involving stool consistency, rectal capacity and sensation, antiperistaltic movement within the rectosigmoid junction, rectal evacuatory function, pelvic floor muscles, internal and external anal sphincter muscles, and the central nervous system (9, 10). The pathophysiology of FI includes pelvic floor dysfunction, anal sphincter weakness, rectal sensorimotor dysfunction (11, 12), and impaired rectal evacuation (4, 13–15). More than one pathophysiological mechanism may contribute to FI in the same patient. The etiologies of FI often involve anal sphincter weakness, which is often due to immediate or delayed muscle or nerve damage from childbirth and complications from prior anorectal surgery. Advanced age also contributes to the diminished function of the pelvic floor and anal sphincter muscles, predisposing the elderly people to FI (16). In addition, bowel habit disturbances and changes in stool consistency play an important role in FI.
A number of exercises involving various pelvic floor muscles, including repetitive voluntary contractions of the external anal sphincter (EAS) muscles such as Kegel exercises, have been clinically used to improve FI (17). Kegel exercises are specific but simple exercises used to restore pelvic floor and sphincter muscle tone and strength. Studies have shown that Kegel exercises can increase anal squeeze pressure, shorten pelvic floor muscle length, and narrow the levator hiatus (9). Kegel exercises are usually combined with electromyography (EMG) or manometry to provide visual feedback. Currently, there is no standardized method of rehabilitative exercise for FI, which results in a heterogeneous mixture of clinical outcomes, conclusions, and recommendations (9, 18).
A potential shortcoming of Kegel exercises is the emphasis on muscle strengthening by squeezing the anal sphincter muscles without involving resistance training. Muscle overload and subsequent neuromuscular fatigue are necessary requirements for any successful strength training, as shown in rehabilitative exercises of other muscle groups such as the limbs, pharyngeal muscles, and suprahyoid upper esophageal sphincter (UES) opening muscles (18–22). Neuromuscular fatigue is defined as an acute exercise-induced reduction in force and is a sign that muscle overload is occurring during exercise (23). The training cycle achieves improvement in direct proportion to the physical work done up to an end point when fatigue occurs in the targeted muscle (18). Progression in resistance training is necessary to reach an adequate training goal (24). To achieve optimal training results, it is important for us to be able to estimate the amount of workload that a patient needs to complete during resistance training before fatigue occurs. Through modulation of the workload, a periodized training plan can enhance the recovery adaption process and eventual performance capacity. Thus far, there is no study to document neuromuscular fatigue during anal sphincter resistance training (25, 26).
Rehabilitation physiology of the pelvic floor, as it pertains to fecal incontinence, is a developing field. For example, despite significant clinical and patient care relevance, basic information such as muscle fatigue induced by pelvic floor exercises has not been systematically studied. This information is crucial for devising novel or modifying existing rehabilitative exercises targeting the continence muscles. For this reason, we aimed to determine the fatigability of the external anal and puborectalis muscles (PRM) involved in fecal continence and hypothesized that applying a compressible resistance during voluntary contraction of the anal sphincter will overload the sphincter muscles, resulting in neuromuscular fatigue of these muscles, manifested by reduction of contractile force.
In the current study, we used a novel apparatus that provides a compressible load allowing for muscle shortening during contraction, the continence muscles Resistance Exerciser Device (cRED), combined with pelvic floor exercises to increase the workload of the muscles involved in anal resting and squeeze pressure.
METHODS
Subjects
We studied 12 healthy (age = 21 ± 2.7 yr) nulliparous female volunteers. All volunteers denied any history of anorectal symptoms and had normal bowel habits. Studies were approved by the Internal Review Board of the Human Research Protection Program at the Medical College of Wisconsin (Milwaukee, WI). All participants gave written informed consent before the studies.
Continence Muscle Resistance Exerciser Device
The handmade continence muscle Resistance Exerciser Device was developed in our laboratory (Fig. 1). The cRED consists of a 6-cm × 2-cm noncompliant cylindrical balloon (intra-anal balloon) that is connected to a small compliant balloon (external balloon) by a 2-mm-diameter tube and a stopcock to allow for air to be filled and sealed in the system. To ensure consistent resistance was provided by the device, a commercially available noncompliant valvuloplasty balloon (Z-Med, Braun Interventional Systems, Inc.) was chosen to serve as the intra-anal balloon in the cRED. The external balloon was handmade using the material from nitrile gloves. The balloon size was same for all the studies. The system was prefilled with air to determine the amount of air needed for an internal pressure or desired resistance of the intra-anal balloon. This was determined using a sphygmomanometer gauge in a sealed system. For the present study, we determined the air needed for an internal pressure of 50 mmHg. The intra-anal balloon, while providing resistance, is compressed by the anal contraction (exceeding 50 mmHg pressure) due to displacement of its air to the external distensible balloon. The compressibility of the anal balloon allows for the muscle shortening necessary for isotonic exercise. Air displacement into the external balloon results in its expansion and serves as an externally visible indicator that an anal contraction has occurred. Using this device, we increased the load on the continence muscles during anal contraction by providing resistance to the striated muscles involved in contraction of the anal canal including the EAS muscles and PRM. The device was assembled by the same laboratory technique and ensured that there was no leakage before use.
Figure 1.

Continence muscle resistance exerciser device.
High-Resolution Anal Manometry
Anorectal manometric pressures were monitored using a high-resolution esophageal manometry catheter (Manoview, Medtronic, Duluth, GA) positioned across the anal canal with the distal end in the rectum. A computerized recording and analysis system (ManoScan Medtronic, Duluth, GA) stores pressure data from 36 sensors spaced 1 cm apart on the manometry catheter. We used the first 8–10 pressure sensors along the manometry catheter for the purposes of this study. The catheter was placed such that at least two or three pressure sensors were positioned in the rectum.
Experimental Protocol
All subjects were placed in the left lateral decubitus position for the duration of the study. Before initiation of the exercise protocol, all subjects were educated on the proper squeeze technique of the anal sphincter. Participants were instructed to squeeze the muscles around the anus with the feeling of anal canal closure and tightening. They were also instructed not to contract their abdomen or buttocks. All subjects then had a digital rectal examination (DRE) and were asked to perform anal squeezes as instructed during DRE. We ensured that every subject could perform the anal squeezes correctly before initiating the study protocol. After applying lubricating gel along the catheter, the catheter was gently placed inside the anal canal with the distal end in the rectum. This allowed for pressure sensors to be arranged along the entire anal canal. After placement of the catheter, a 5-min interval was allotted before the start of the exercise protocol to allow the sphincter tone to return to the basal level. Subjects were verbally cued to perform anal contractions with and without a resistance load provided by the cRED.
The intra-anal balloon of the cRED was introduced only in exercises when a resistive load was applied. For these exercises, it was placed in a deflated state parallel to the manometric catheter with the distal end of the balloon just beyond the anal margin. The balloon was then inflated to the desired resistance of 50 mmHg. Small adjustments of the balloon position were sometimes necessary after inflation to ensure the balloon straddled the high-pressure zone of the anal canal. After position adjustment, the catheter of the cRED was taped to perianal skin to minimize sliding of the device. When subjects squeezed the intra-anal balloon correctly, the expansion of the external balloon could be clearly visualized, and this was used to educate the volunteers about performing the anal contraction correctly. For exercise without a load, the anal balloon was not placed.
Two types of exercises were performed, namely, repetitive short squeeze contractions and long squeeze contractions. Each set of repetitive short squeeze contractions consisted of 40 consecutive 3-s anal contractions alternating with 3-s rest. For long squeeze contractions, subjects were instructed to perform one continuous squeeze of the anus for up to 30 s. Under each exercise condition (with or without a load), the subjects performed exercises in the following sequence: two long squeeze contractions with 1-min rest in between followed by one set of repetitive short squeeze contractions after another 1-min rest. Considering the higher chance of introducing variability in manometric recording with placing an anal load compared with that without a load, the anal contraction exercises with a resistive load were repeated one more time. There was an 8-min rest after completing a set of repetitive short squeeze contractions. The exercises with and without a load were in a randomized order determined before the exercises by flipping a coin, such that all exercises with a load were performed either in the beginning or end depending on the randomization. Figure 2 illustrates the randomization and sequence of exercises.
Figure 2.

Schematic diagram of the study protocol.
Manometric Parameters of Fatigue
Two manometric parameters, namely, maximum squeeze pressure and anal squeeze contractile integral (CI), were measured and analyzed for each anal contraction. These measures were used to determine presence or absence of fatigue. They were obtained using the “Smart Mouse” feature in the Manoview analysis software. The CI is an estimate of the total pressure throughout the length of the high-pressure zone (HPZ) and the duration of the contraction. It is obtained by multiplying the mean pressure amplitude by the contraction duration by the length of interest. For the present study, the HPZ was delineated by a pressure above 20 mmHg using the isobaric contour function of the analysis software, similar to previous studies involving the distal esophagus (27). The Smart Mouse was then used to form a space-time box around the area of interest in the topographic pressure display to determine the CI (Fig. 3). The CI has been used in anorectal manometry (28), the distal esophagus (27), and pharynx (22) as a metric for “contractile vigor.” For the present study, the CI and maximum pressure of the 40 repetitive short squeeze contractions were grouped into eight epochs, each consisting of five contractions. The average anal CI and maximum squeeze pressure within each epoch were used as manometric surrogates for detecting fatigue due to repeated anal contractions against the increased load provided by the cRED. The maximum anal sphincter pressure at rest at any level in the anal canal is defined as the resting sphincter pressure.
Figure 3.

Space-time box showing the contractile integral of the anal contraction on the Manoview analysis software.
Fatigue rate (FR) is the rate at which the squeeze pressure of the EAS reduces per minute (29–31). It is a simple measurement and has been used to assess external anal sphincter function. The fatigue rate (FR) was calculated using the first 20 s of the long squeeze contraction pressure data. The pressure measurements after the peak pressure point were recorded using the maximum pressure at each time point (every 0.01 s). The equation of the best-fit line for the fatigability tracing was obtained by linear regression (29). The slope of the pressure over the 20 s of long squeeze contraction provided the value of the FR.
Statistical Analysis
A paired t test was used to compare the difference of baseline resting pressure and maximum squeeze pressure with and without a resistive load. Repeated two-way analysis of variance was used to detect decreasing CI and maximum squeeze pressure during the 40 repetitive short squeeze contractions in eight epochs. Slope values were compared for these parameters with and without the application of a resistive load, the cRED, by using a paired t test. The FR was calculated by linear regression during the 20-s long squeeze contraction period and compared both with and without a load by a paired t test. Data are presented as means ± SE, unless otherwise stated.
All authors had access to the study data and reviewed and approved the final manuscript.
RESULTS
The experimental procedure was well tolerated by all subjects without any adverse events. The baseline resting pressure and maximum squeeze pressure were significantly higher with application of an anal resistive load compared with that without a load (resting sphincter pressure = 96 ± 12 mmHg vs.76 ± 7 mmHg, P < 0.01; maximum squeeze pressure = 198 ± 60 mmHg vs.158 ± 57 mmHg, P < 0.01). The findings that the resting pressure and maximum squeeze pressure were higher with the anal balloon in place were expected, as the contact pressure resulting from the inflated intra-anal balloon increased the overall measurement of anal canal pressures. In addition, earlier studies in humans and rabbits suggest that EAS muscles operate at a short sarcomere length, which is below the optimal muscle length (32–34). As the intra-anal balloon of the cRED distended the anal canal, it may result in an increased EAS sarcomere length and thus contribute to increased anal canal pressures at rest and during squeeze.
Repetitive Short Squeeze Anal Contraction with a Load
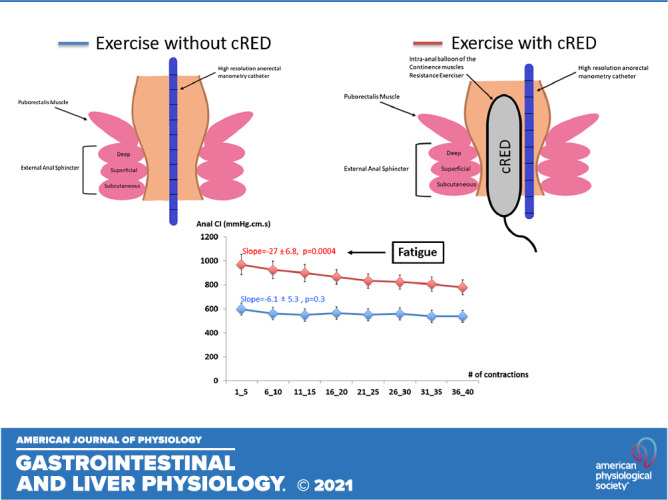
Repetitive contraction against a resistive load showed significant decrease in anal CI (P < 0.0001) and maximum squeeze pressure (P < 0.0001). Linear regression analysis showed a significant negative correlation between anal CI pressure and successive contraction against a load (Fig. 4, slope = −27, P = 0.0004), suggesting “muscle fatigue”. This was consistently observed in 75% (9 out of 12) of the subjects. The remaining three subjects failed to show signs of fatigue (regression slope = 4.3, −6.2, and −6.7, respectively, P > 0.05). Similar findings were observed for maximum squeeze pressure (Fig. 5, slope = −4.2, P = 0.0003). In further pairwise comparisons among epochs (e.g., epoch 1 vs. epoch 2, epoch 1 vs. epoch 3, etc.), despite progressive decline in anal CI from epoch 1 to epoch 8, significant decrease of anal CI started at epoch 5 compared with epoch 1. For maximum squeeze pressure, significant decline started at epoch 4. Therefore, the results suggested that fatigue occurred after subjects completed almost half of the 40 repetitive short squeeze anal contractions.
Figure 4.

Change of anal contractile integral (anal CI ± SE) over 40 consecutive anal squeeze exercises, no load vs. with load. N = 12 subjects. The y-axis is the anal contractile integral (mmHg·cm·s), and the x-axis is the order of contractions, which are grouped into 8 epochs. Data were analyzed using repeated two way analysis of variance. Consecutive anal squeeze against a resistive load showed significant decrease in anal CI (P < 0.0001). Linear regression analysis showed a significant negative correlation between anal CI and successive squeeze exercise against load. There was no significant change in anal CI during exercise without load.
Figure 5.

Change of anal maximum squeeze pressure (max ± SE) over 40 consecutive anal squeeze exercises, no load vs. with load. N = 12 subjects. The y-axis is the anal maximum squeeze pressure (mmHg), and the x-axis is the order of contractions, which are grouped into 8 epochs. Data were analyzed using repeated two way analysis of variance. Consecutive anal squeeze against a resistive load showed significant decrease in maximum anal squeeze pressure (P < 0.0001). Linear regression analysis showed a significant negative correlation between maximum anal squeeze pressure and successive squeeze exercise against load. There was no significant change in maximum anal squeeze pressure during exercise without load.
Repetitive Short Squeeze Anal Contraction without a Load
Contrary to the findings with a load, there was no significant change in anal CI or maximum squeeze pressure during the 40 contractions without a load (Figs. 4 and 5). Pairwise comparisons among epochs without application of a resistive load did not show any significant difference in the anal CI during the 40 consecutive contractions. This suggested that repetitive short squeeze anal contractions without a load failed to achieve “muscle fatigue.”
Long Squeeze Anal Contraction with and without a Load
Fatigue rate was significantly more negative during long squeeze contraction against a resistive load than without a load (−40 ± 5 mmHg/20 s vs. −16 ± 5 mmHg/20 s, P = 0.0002). Figure 6 shows paired plot data of the individual’s FR, with load compared with without load. Thus, long squeeze contraction against a load was more susceptible to fatigue than that without a load.
Figure 6.

Paired plot data of the individual’s FR, no load vs. with load. N = 12 subjects. Data were analyzed using paired t test. The y-axis represents the pressure change in 20 s. FR was significantly more negative in sustained squeeze against a resistive load than without load. FR, fatigue rate.
DISCUSSION
In this study, we demonstrated that the application of a resistive load to the anal canal during repetitive short squeeze contractions could effectively fatigue the anal sphincter muscles, as evidenced by a progressive reduction in the anal CI and the maximum squeeze pressure. Notably, repetitive short squeeze anal contractions without a load failed to show signs of fatigue by the end of the 40 repetitive short squeeze contractions. Furthermore, long squeeze anal contraction against a resistive load resulted in more rapid muscle fatigue compared with no load. The results of this study indicate that to achieve neuromuscular fatigue, it is important to increase the working load for the sphincter muscles during anal rehabilitative exercise.
Anal sphincter weakness is one of the most common reasons for fecal incontinence. Pelvic floor exercises that involve squeezing the anal sphincter with or without biofeedback are the mainstay of noninvasive treatment options to improve the contractile function of the anal sphincter. The EAS along with the PRM is a major contributor to the anal squeeze pressure. As striated muscles, they are theoretically amenable to the same training techniques as other skeletal muscles (17). Kegel exercises are the most widely used pelvic floor exercises for fecal and urinary incontinence, which were introduced by Dr. Arnold Kegel in 1948 (35, 36). However, since their introduction, there have been significant variations of the training regimens used in terms of the type, number, and intensity of exercises. There is a lack of consensus on how many contractions and the length of time of contractions that should be performed daily. According to the literature, the recommendations for pelvic floor muscle contractions extend from 5 to 200 per day (18).
To date, there have been no studies in the literature designed to prove the occurrence of muscle fatigue during anal rehabilitative training. There are limited studies introducing resistance training into an anal exercise regimen in patients with fecal incontinence. Resistance training with a saline filled bag for 6 wk has been shown to increase maximum squeeze pressure in three patients with FI (37). Resistance training with an inflatable probe and home biofeedback has been shown to also increase maximum squeeze pressures (38). Neither of these studies evaluated sphincter muscle fatigue with resistance training.
In resistance training, the targeted muscle needs to perform more work to overcome a predetermined force generated by resistance (24, 39). This type of training results in an increased number and size of mitochondria, enhanced activity of some aerobic and anaerobic enzymes, increased intramuscular glycogen content, and an increased number of capillaries and their surface area (18, 40). This eventually leads to muscle hypertrophy (18, 41). To induce resistance to anal contraction, we developed a device that is designed to overload the anal sphincter muscles, and by being compressible, it allows the anal sphincter muscles to shorten, mimicking normal function. We used a task-specific strength training approach by creating a predetermined amount of resistance during anal contractions and confirmed the hypothesis that anal contraction against resistance resulted in fatigue of the anal sphincter, as shown in decline of maximum squeeze pressure and CI.
It is known that the EAS consists of a mosaic of type I and type II muscle fibers. The EAS is predominantly composed of type I, slow-twitch, fatigue-resistant fibers that enable the muscle to maintain a long squeeze tonic contraction (42). Similar to other skeletal muscles, there is a preferential denervation of fast-twitch fibers, leading to a higher proportion of slow-twitch fibers with age (30). Thus, the EAS is more resistant to fatigue with increasing age. Previous studies have shown that patients with a weak EAS are less susceptible to fatigue during long squeeze contractions, which could attribute to a higher proportion of slow-twitch muscle fibers in the EAS (30, 43). Fatigue resistance is an important mechanism to maintain continence. This fatigue resistance may pose a challenge to successful rehabilitative exercise of the EAS since neuromuscular fatigue is a prerequisite before a muscle can be strengthened. This implies that it is necessary to overload the anal sphincter muscles for contraction exercise to be effective. Moreover, an earlier study shows central fatigue mechanisms during sustained voluntary contraction of the EAS (44). It suggests that the observed decline in voluntary activation of anal sphincter muscles during fatiguing contractions is possibly driven by central fatigue rather than peripheral fatigue. This means that anal sphincter muscles would be unlikely to be loaded sufficiently to induce hypertrophy during sustained efforts (44). Thus, it further supports the concept of overload during anal sphincter rehabilitative training. In the current study, we evaluated long squeeze contractions against a resistive load. The results demonstrate increased fatigability of the anal sphincter with the application of a load, as evidenced by a significantly more negative FR compared with that without a load. This finding further confirms the effectiveness of the present exercise protocol.
Our study has several limitations. First, in this study, our subjects were all healthy, young, and nulliparous females. In this study, we noticed that 25% of the participants failed to show fatigue of anal sphincter muscles after 40 repetitive short squeeze contraction exercises with a resistive load. This could be due to inadequate muscle load for those subjects, as healthy subjects may require a high resistive load to achieve fatigue with our exercise protocol. This population was chosen for the pilot study because it is essential to understand the normal muscle physiology and fatigability of the anal sphincter with anal rehabilitative exercises before expanding to other populations. Second, since this is a pilot study, the magnitude of the resistance load and the number of repetitions were empirically determined. However, the findings of the current study pave the way for future studies to explore different loads and number of repetitions in patients with fecal incontinence. Third, it is known that the EAS combined with the PRM contribute to the anal squeeze pressure. It is difficult to separate these two muscles based on manometric profiles; however, there are studies suggesting voluntary contractions of the PRM and the EAS increase pressure in the proximal and distal halves of the anal canal, respectively (45, 46). Thus, we do not know whether the fatigue is driven by the EAS alone or with the PRM. Earlier studies have shown that contraction of the PRM contributes to the vaginal HPZ on vaginal manometry (47, 48). Future studies with vaginal manometry may help to delineate the role of the PRM in exercise-induced fatigue. Finally, one may argue that placement of an inflated balloon in the anal canal will affect the manometry recordings of the true pressure profile; however, since we are performing intrasubject comparisons and the variation is consistent during the study on each subject, it should not affect our conclusions.
The findings in this study could potentially enhance the pelvic biofeedback training, as the external balloon of the cRED serves as a visual feedback of anal squeeze contraction exercises. With an appropriate anal contraction, the external balloon expands and the degree of expansion is an indirect indicator for contraction strength. During pelvic training in fecal incontinence, patients are able to titrate the anal resistive training load by adjusting the internal pressure of the cRED based on their muscle performance to enhance muscle regrowth and function.
In summary, short and long squeeze contractions against a compressible load induce fatigue and thus have the potential to strengthen the anal sphincter contractile function than contractions without a load. These results provide insight on future therapeutic approaches for fecal incontinence in clinical practice.
GRANTS
This work was supported by National Institute of Diabetes and Digestive and Kidney Diseases Grants P01DK068051 and T32DK061923.
DISCLOSURES
No conflicts of interest, financial or otherwise, are declared by the authors.
AUTHOR CONTRIBUTIONS
L.M., K.P., P.S., and R.S. conceived and designed research; L.M., K.P., N.L., and A.B. performed experiments; L.M. and K.P. analyzed data; L.M., K.P., M.K.K., A.B., P.S., and R.S. interpreted results of experiments; L.M., K.P., and M.K.K. prepared figures; L.M., K.P., and M.K.K. drafted manuscript; P.S. and R.S. edited and revised manuscript; R.S. approved final version of manuscript.
REFERENCES
- 1.Bharucha AE, Dunivan G, Goode PS, Lukacz ES, Markland AD, Matthews CA, Mott L, Rogers RG, Zinsmeister AR, Whitehead WE, Rao SS, Hamilton FA. Epidemiology, pathophysiology, and classification of fecal incontinence: state of the science summary for the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) workshop. Am J Gastroenterol 110: 127–136, 2015. doi: 10.1038/ajg.2014.396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Macmillan AK, Merrie AEH, Marshall RJ, Parry BR. The prevalence of fecal incontinence in community-dwelling adults: a systematic review of the literature. Dis Colon Rectum 47: 1341–1349, 2004. doi: 10.1007/s10350-004-0593-0. [DOI] [PubMed] [Google Scholar]
- 3.Ditah I, Devaki P, Luma HN, Ditah C, Njei B, Jaiyeoba C, Salami A, Ditah C, Ewelukwa O, Szarka L. Prevalence, trends, and risk factors for fecal incontinence in United States adults, 2005-2010. Clin Gastroenterol Hepatol 12: 636–643, 2014. doi: 10.1016/j.cgh.2013.07.020. [DOI] [PubMed] [Google Scholar]
- 4.Whitehead WE, Borrud L, Goode PS, Meikle S, Mueller ER, Tuteja A, Weidner A, Weinstein M, Ye W; Pelvic Floor Disorders Network. Fecal incontinence in US adults: epidemiology and risk factors. Gastroenterology 137: 512–517, 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Saldana Ruiz N, Kaiser AM. Fecal incontinence—Challenges and solutions. World J Gastroenterol 23: 11–24, 2017. doi: 10.3748/wjg.v23.i1.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bharucha AE, Zinsmeister AR, Locke GR, Schleck C, McKeon K, Melton LJ. Symptoms and quality of life in community women with fecal incontinence. Clin Gastroenterol Hepatol 4: 1004–1009, 2006. doi: 10.1016/j.cgh.2006.01.003. [DOI] [PubMed] [Google Scholar]
- 7.Bharucha AE, Zinsmeister AR, Locke GR, Seide BM, McKeon K, Schleck CD, Melton LJ. Prevalence and burden of fecal incontinence: a population-based study in women. Gastroenterology 129: 42–49, 2005. doi: 10.1053/j.gastro.2005.04.006. [DOI] [PubMed] [Google Scholar]
- 8.Perry S, Shaw C, McGrother C, Matthews RJ, Assassa RP, Dallosso H, Williams K, Brittain KR, Azam U, Clarke M, Jagger C, Mayne C, Castleden CM; Leicestershire MRC Incontinence Study Team. Prevalence of faecal incontinence in adults aged 40 years or more living in the community. Gut 50: 480–484, 2002. doi: 10.1136/gut.50.4.480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.McLemore EC, Sands DR. Biofeedback Therapy (Neuromuscular Training) for fecal incontinence. In: GI Motility Testing: a laboratory and office handbook, edited by Parkman HP, McCallum RW and Rao SS, p. 189–197. [Google Scholar]
- 10.Palit S, Lunniss PJ, Scott SM. The physiology of human defecation. Dig Dis Sci 57: 1445–1464, 2012. doi: 10.1007/s10620-012-2071-1. [DOI] [PubMed] [Google Scholar]
- 11.Chan CLH, Lunniss PJ, Wang D, Williams NS, Scott SM. Rectal sensorimotor dysfunction in patients with urge faecal incontinence: evidence from prolonged manometric studies. Gut 54: 1263–1272, 2005. doi: 10.1136/gut.2005.071613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Mundet L, Cabib C, Ortega O, Rofes L, Tomsen N, Marin S, Chacon C, Clave P. Defective conduction of anorectal afferents is a very prevalent pathophysiological factor associated to fecal incontinence in women. J Neurogastroenterol Motil 25: 423–435, 2019. doi: 10.5056/jnm18196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bharucha AE, Zinsmeister AR, Locke GR, Seide BM, McKeon K, Schleck CD, Melton LJ 3rd.. Risk factors for fecal incontinence: a population-based study in women. Am J Gastroenterol 101: 1305–1312, 2006. [DOI] [PubMed] [Google Scholar]
- 14.Swash M, Snooks SJ, Henry MM. Unifying concept of pelvic floor disorders and incontinence. J R Soc Med 78: 906–911, 1985. doi: 10.1177/014107688507801105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Vollebregt PF, Wiklendt L, Dinning PG, Knowles CH, Scott SM. Coexistent faecal incontinence and constipation: a cross-sectional study of 4027 adults undergoing specialist assessment. EClinicalMedicine 27: 100572, 2020. doi: 10.1016/j.eclinm.2020.100572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Yu SWB, Rao SSC. Anorectal physiology and pathophysiology in the elderly. Clin Geriatr Med 30: 95–106, 2014. doi: 10.1016/j.cger.2013.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Norton C, Cody JD, Hosker G. Biofeedback and/or sphincter exercises for the treatment of faecal incontinence in adults. Cochrane Database Syst Rev, 7: 2012. CD002111. doi: 10.1002/14651858.cd002111.pub3. [DOI] [PubMed] [Google Scholar]
- 18.Marques A, Stothers L, Macnab A. The status of pelvic floor muscle training for women. Can Urol Assoc J 4: 419–424, 2010. doi: 10.5489/cuaj.10026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Agrawal D, Kern M, Edeani F, Balasubramanian G, Hyngstrom A, Sanvanson P, Shaker R. Swallow strength training exercise for elderly: a health maintenance need. Neurogastroenterol Motil 30: e13382, 2018. doi: 10.1111/nmo.13382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.McArdle WD, Katch FI, Katch VL. Essentials of Exercise Physiology. New York, NY: Williams & Wilkins, 2010. [Google Scholar]
- 21.Shaker R, Easterling C, Kern M, Nitschke T, Massey B, Daniels S, Grande B, Kazandjian M, Dikeman K. Rehabilitation of swallowing by exercise in tube-fed patients with pharyngeal dysphagia secondary to abnormal UES opening. Gastroenterology 122: 1314–1321, 2002. doi: 10.1053/gast.2002.32999. [DOI] [PubMed] [Google Scholar]
- 22.Shaker R, Sanvanson P, Balasubramanian G, Kern M, Wuerl A, Hyngstrom A. Effects of laryngeal restriction on pharyngeal peristalsis and biomechanics: clinical implications. Am J Physiol Gastrointest Liver Physiol 310: G1036–G1043, 2016. doi: 10.1152/ajpgi.00010.2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gandevia SC. Spinal and supraspinal factors in human muscle fatigue. Physiol Rev 81: 1725–1789, 2001. doi: 10.1152/physrev.2001.81.4.1725. [DOI] [PubMed] [Google Scholar]
- 24.Kraemer WJ, Adams K, Cafarelli E, Dudley GA, Dooly C, Feigenbaum MS, Fleck SJ, Franklin B, Fry AC, Hoffman JR, Newton RU, Potteiger J, Stone MH, Ratamess NA, Triplett-McBride T; American College of Sports Medicine. American college of sports medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc 34: 364–380, 2002. doi: 10.1097/00005768-200202000-00027. [DOI] [PubMed] [Google Scholar]
- 25.Haff GG. Quantifying workloads in resistance training: a brief review. Strength Cond J 10: 31–40, 2010. [Google Scholar]
- 26.Halson SL. Monitoring training load to understand fatigue in athletes. Sports Med 44, Suppl 2: S139–S147, 2014. doi: 10.1007/s40279-014-0253-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lin Z, Roman S, Pandolfino JE, Kahrilas PJ. Automated calculation of the distal contractile integral in esophageal pressure topography with a region-growing algorithm. Neurogastroenterol Motil 24: e4–e10, 2012. doi: 10.1111/j.1365-2982.2011.01795.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Carrington EV, Knowles CH, Grossi U, Scott SM. High-resolution anorectal manometry measures are more accurate than conventional measures in detecting anal hypocontractility in women with fecal incontinence. Clin Gastroenterol Hepatol 17: 477–485.e9, 2019. doi: 10.1016/j.cgh.2018.06.037. [DOI] [PubMed] [Google Scholar]
- 29.Marcello PW, Barrett RC, Coller JA, Schoetz DJ Jr, Roberts PL, Murray JJ, Rusin LC. Fatigue rate index as a new measurement of external sphincter function. Dis Colon Rectum 41: 336–343, 1998. doi: 10.1007/BF02237488. [DOI] [PubMed] [Google Scholar]
- 30.Nockolds CL, Hosker GL, Kiff ES. Fatigue rate of the external anal sphincter. Colorectal Dis 14: 1095–1100, 2012. doi: 10.1111/j.1463-1318.2011.02901.x. [DOI] [PubMed] [Google Scholar]
- 31.Telford KJ, Ali ASM, Lymer K, Hosker GL, Kiff ESHill J. Fatigability of the external anal sphincter in anal incontinence. Dis Colon Rectum 47: 746–752, 2004. doi: 10.1007/s10350-003-0122-6. [DOI] [PubMed] [Google Scholar]
- 32.Mittal RK, Sheean G, Padda BS, Lieber R, Raj Rajasekaran M. The external anal sphincter operates at short sarcomere length in humans. Neurogastroenterol Motil 23: 643–e258, 2011. doi: 10.1111/j.1365-2982.2011.01700.x. [DOI] [PubMed] [Google Scholar]
- 33.Rajasekaran MR, Jiang Y, Bhargava V, Lieber RL, Mittal RK. Novel applications of external anal sphincter muscle sarcomere length to enhance the anal canal function. Neurogastroenterol Motil 23: 70–75, 2011. doi: 10.1111/j.1365-2982.2010.01608.x. [DOI] [PubMed] [Google Scholar]
- 34.Rajasekaran MR, Jiang Y, Bhargava V, Littlefield R, Lee A, Lieber RL, Mittal RK. Length-tension relationship of the external anal sphincter muscle: implications for the anal canal function. Am J Physiol Gastrointest Liver Physiol 295: G367–G373, 2008. doi: 10.1152/ajpgi.00033.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kegel AH. Progressive resistance exercise in the functional restoration of the perineal muscles. Am J Obstet Gynecol 56: 238–248, 1948. doi: 10.1016/0002-9378(48)90266-x. [DOI] [PubMed] [Google Scholar]
- 36.Siff LN, Hill AJ, Walters SJ, Walters G, Walters MD. The effect of commonly performed exercises on the levator hiatus area and the length and strength of pelvic floor muscles in postpartum women. Female Pelvic Med Reconstr Surg 26: 61–66, 2020. doi: 10.1097/SPV.0000000000000590. [DOI] [PubMed] [Google Scholar]
- 37.Tuttle L, Kunkel D, Mittal R. Functional lumen imaging probe (FLIP) to perform biofeedback and strengthening of the anal canal muscles. 154: S549–S550, 2018. doi: 10.1016/S0016-5085(18)32038-9. [DOI] [Google Scholar]
- 38.Sharma A, Xiang X, Yan Y, Patcharatrakul T, Parr R, Herekar A, Ayyala DN, Rao SS. Home biofeedback therapy with novel device versus office biofeedback therapy for fecal incontinence: randomized controlled study. Gastroenterology. 156: S-164–S-165, 2019. doi: 10.1016/S0016-5085(19)37203-8. [DOI] [Google Scholar]
- 39.Delorme TL, Watkins AL. Technics of progressive resistance exercise. Arch Phys Med Rehabil 29: 263–273, 1948. [PubMed] [Google Scholar]
- 40.Hollmann W. Preventative cardiology and physical activity. In: The physiology and pathophysiology of exercise tolerance, edited by Steinacker JW and Ward SA.. New York and London: Plenum Press, 1996. [Google Scholar]
- 41.Russel B, Brubaker L. Muscle function and ageing. In: Pelvic Floor Re-education. 2008. New York: Springer, 2008, p. 49–61. [Google Scholar]
- 42.Johnson MA, Polgar J, Weightman D, Appleton D. Data on the distribution of fibre types in thirty-six human muscles. An autopsy study. J Neurol Sci 18: 111–129, 1973. doi: 10.1016/0022-510x(73)90023-3. [DOI] [PubMed] [Google Scholar]
- 43.Cattle KR, Telford K, Kiff ES. Changes in fatigability of the striated anal canal after childbirth. Colorectal Dis 12: 880–884, 2010. doi: 10.1111/j.1463-1318.2009.01875.x. [DOI] [PubMed] [Google Scholar]
- 44.Schabrun SM, Stafford RE, Hodges PW. Anal sphincter fatigue: is the mechanism peripheral or central? Neurourol Urodyn 30: 1550–1556, 2011. doi: 10.1002/nau.21162. [DOI] [PubMed] [Google Scholar]
- 45.Liu J, Guaderrama N, Nager CW, Pretorius DH, Master S, Mittal RK. Functional correlates of anal canal anatomy: puborectalis muscle and anal canal pressure. Am J Gastroenterol 101: 1092–1097, 2006. doi: 10.1111/j.1572-0241.2006.00596.x. [DOI] [PubMed] [Google Scholar]
- 46.Padda BS, Jung S-A, Pretorius D, Nager CW, Den-Boer D, Mittal RK. Effects of pelvic floor muscle contraction on anal canal pressure. Am J Physiol Gastrointest Liver Physiol 292: G565–G571, 2007. doi: 10.1152/ajpgi.00250.2006. [DOI] [PubMed] [Google Scholar]
- 47.Guaderrama NM, Nager CW, Liu J, Pretorius DH, Mittal RK. The vaginal pressure profile. Neurourol Urodyn 24: 243–247, 2005. doi: 10.1002/nau.20112. [DOI] [PubMed] [Google Scholar]
- 48.Raizada V, Bhargava V, Jung S-A, Karstens A, Pretorius D, Krysl P, Mittal RK. Dynamic assessment of the vaginal high-pressure zone using high-definition manometery, 3-dimensional ultrasound, and magnetic resonance imaging of the pelvic floor muscles. Am J Obstet Gynecol 203: e171–178, 2010. 10.1016/j.ajog.2010.02.028 [DOI] [PMC free article] [PubMed] [Google Scholar]