
Figure 1. Risk of total adenoma according to (A) total fructose and (B) sugar-sweetened beverage intake during adolescence by lifestyle and dietary factors in the Nurses’ Health Study II, 1998–2015.
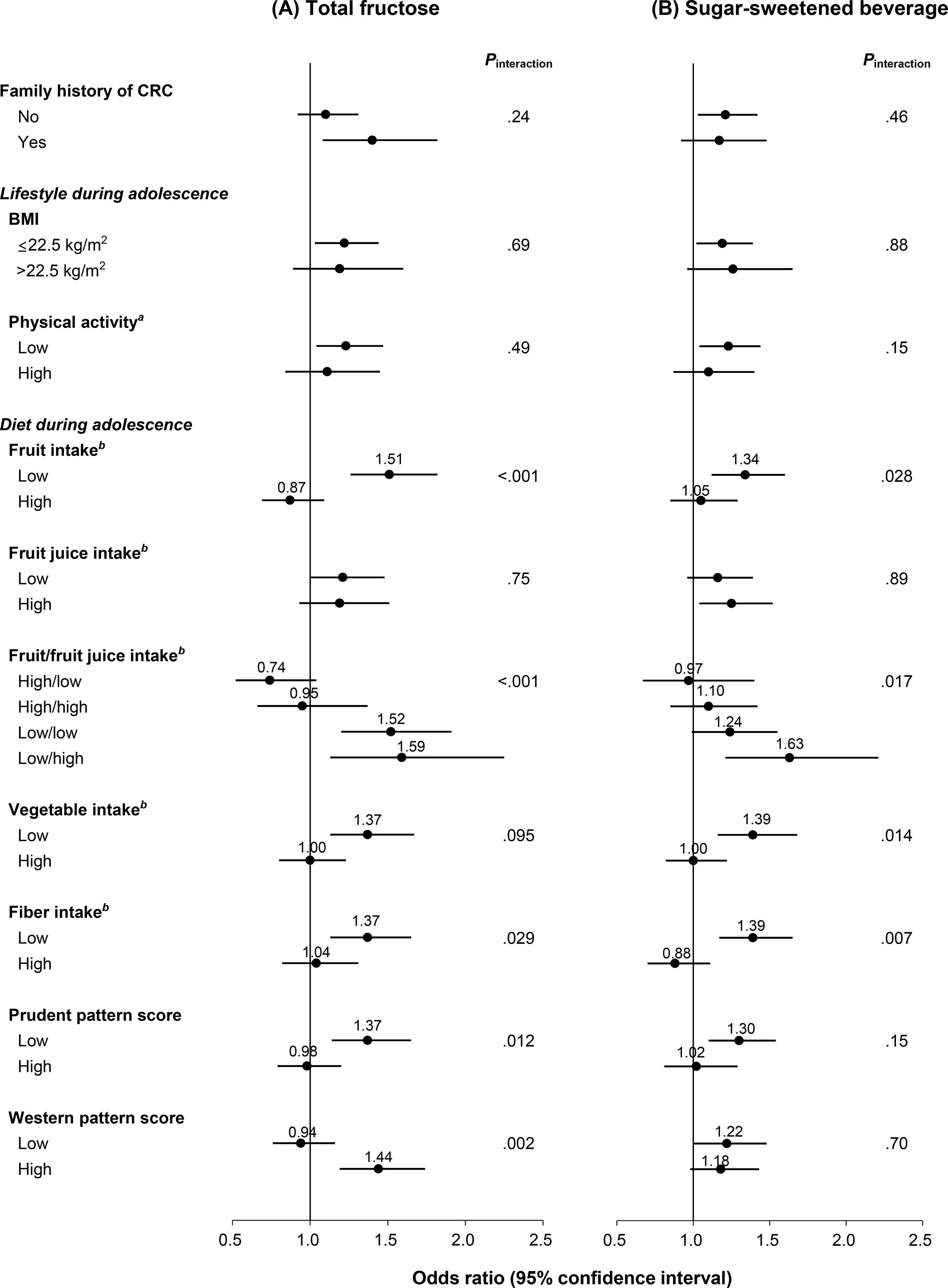
CRC, colorectal cancer; BMI, body mass index
Data were adjusted for age, time period of endoscopy, number of endoscopies, time since most recent endoscopy, reason for endoscopy, family history of CRC, menopausal status/menopausal hormone use, current aspirin use ≥2 times/wk, history of type 2 diabetes, adult height, BMI (age 18 y, current), smoking status (adolescent, current), alcohol consumption (age 18–22 y, current), physical activity (adolescent, current), adolescent and current (adult) dietary intake (total calorie, total calcium, vitamin D, total folate, fiber, fruits, vegetables, and dairy), current total red meat intake, western dietary pattern score during adolescence, and current total fructose or sugar-sweetened beverage intake except for the stratifying variable of each stratum.
(A) highest vs lowest (referent) quintile.
(B) ≥1 serving/d vs <1 serving/wk (referent).
aHigh: highest tertile (≥59 MET-hr/wk); low: two lower tertiles (<59 MET-hr/wk).
bCut-off: median intake (fruits, 1.3 serving/d; fruit juice, 0.4 serving/d; vegetables, 2.8 serving/d; fiber, 20.2 g/d).