
Figure 1.
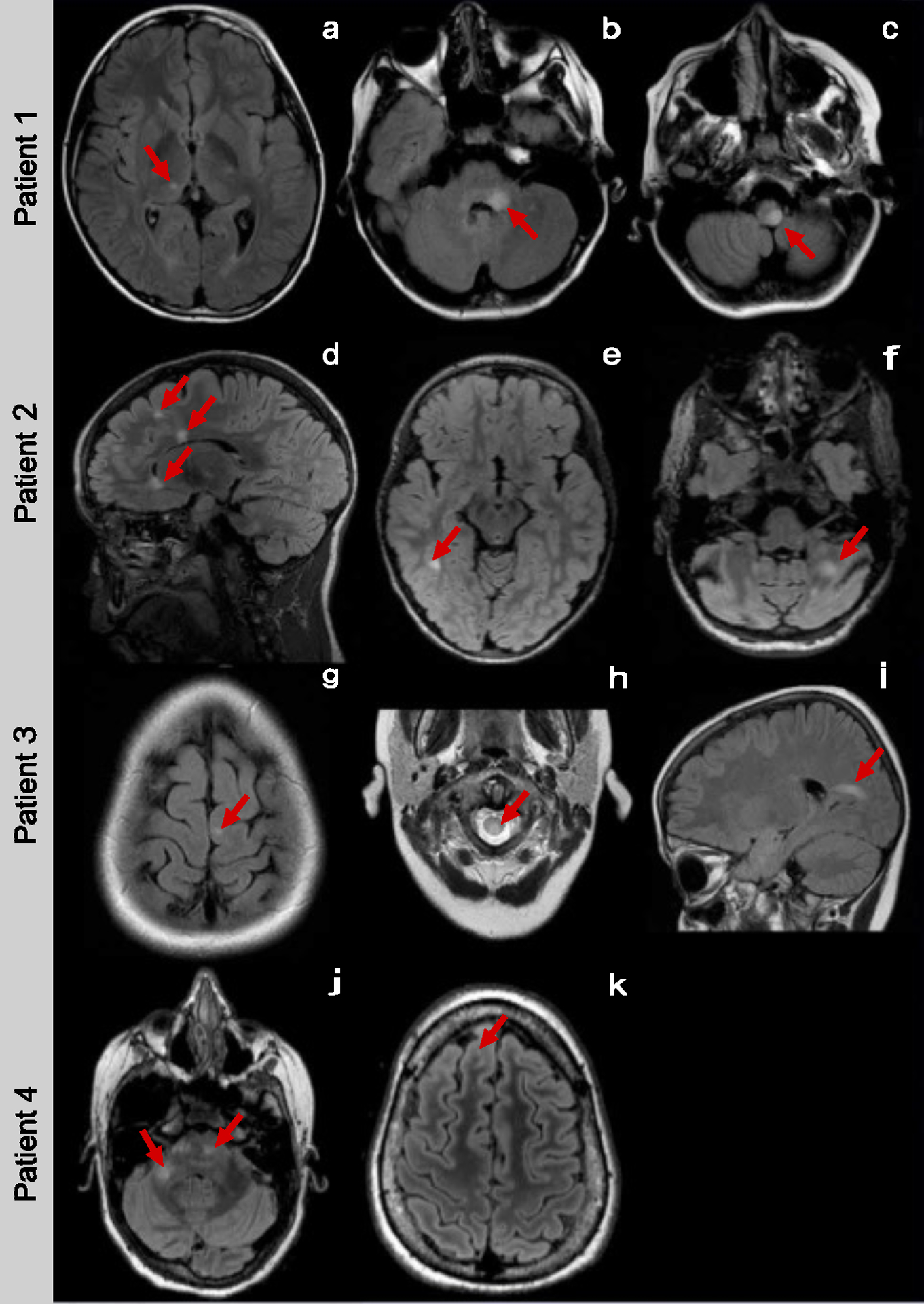
Case 1: An 11-year-old boy presented with facial weakness, double vision and hemiparesis. CSF analysis showed 7 white blood cells (WBCs) per μl, normal glucose, and protein, but no evidence of intrathecal IgG synthesis. His MRI showed deep grey matter, cerebellar peduncle, and partial medullary T2-bright lesions (Figure 1-a, b, c). Six months after the initial presentation, he developed right leg weakness and double vision. Disease activity stopped after initiating natalizumab.
Case 2: A 4-year old girl presented with poor coordination and falls. Her MRI images showed juxtacortical, periventricular, corpus callosum, and cerebellar T2-bright lesions suggestive of MS (Figure 1-d, e, f). CSF analysis showed no WBCs and normal protein and glucose. Intrathecal IgG synthesis was not evaluated. Five months after the initial presentation, she developed right facial weakness and dysarthria. The MRI images and clinical presentation were thought to be compatible with MS. Disease activity stopped after initiating natalizumab.
Case 3: A 10-year-old boy presented with bilateral leg weakness and sphincter dysfunction. CSF results were not available for review. His MRI showed juxtacortical, periventricular, infratentorial, and partial spinal cord T2-bright lesions (Figure 1-g, h, i). Six months after the initial presentation, he developed ataxia, and three months later, he presented with new-onset hand numbness. He started subcutaneous interferon beta-1a, but no further follow-up was available.
Case 4: A 14-year-old girl presented with slurred speech and extremity paresthesia. CSF analysis showed evidence of intrathecal IgG synthesis. Her MRI showed subcortical, pontine, and cerebellar peduncle T2-bright lesions (Figure 1-j, k). Although she had no further clinical attacks, subsequent MRI scans showed new T2-bright lesions. While she had no disease activity on natalizumab, she switched to glatiramer acetate due to safety concerns and remained clinically stable on that treatment.