
FIGURE 2.
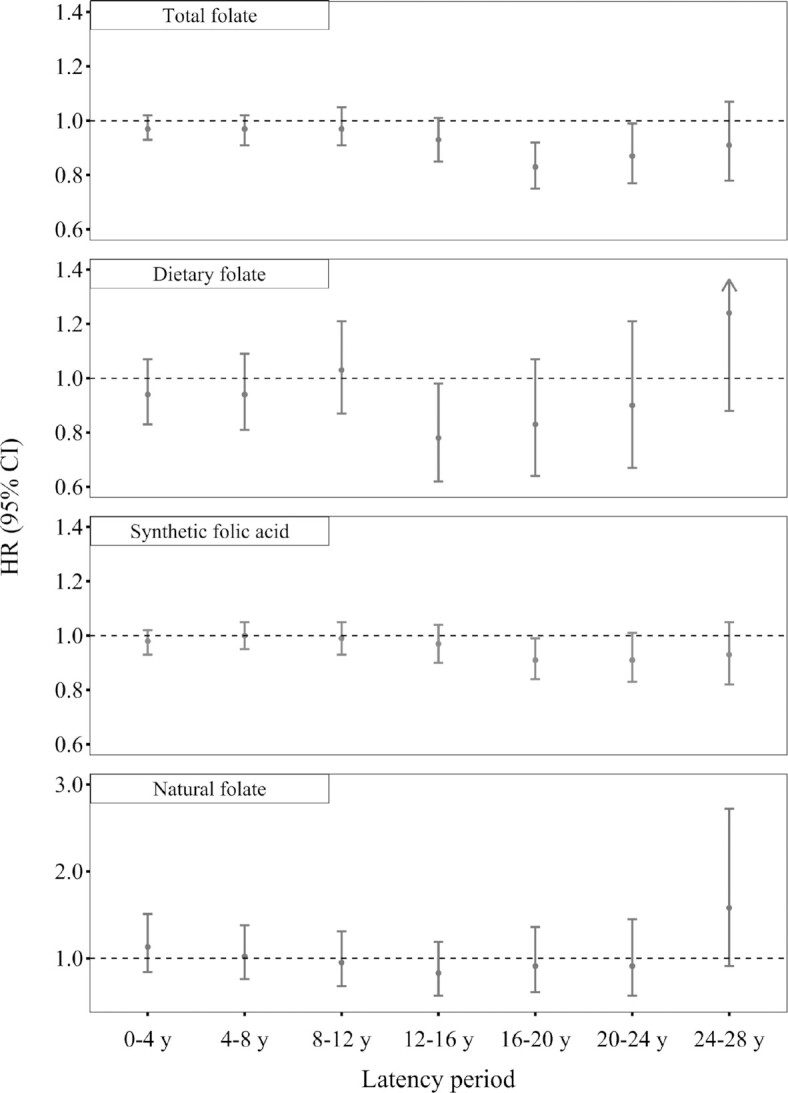
Risk of CRC per 400 DFE/d greater folate intake with different latency periods, Nurses’ Health Study, 1980–2016. Cox models were stratified by age and calendar year and adjusted for family history of CRC, endoscopy, height, BMI, pack-y of smoking before age 30 y, physical activity, duration of regular aspirin/NSAIDs use, duration of multivitamin use (for dietary folate and natural folate analysis), menopausal status and menopausal hormone use, alcohol intake, total energy, dietary fiber, total vitamin D (for total folate and synthetic folic acid analysis), dietary vitamin D (for dietary folate and natural folate analysis), total calcium (for total folate and synthetic folic acid analysis), dietary calcium (for dietary folate and natural folate analysis), red meat, and processed meat. For different latency periods, we used folate intake reported at various latencies (i.e., 4–8, 8–12, 12–16, 16–20, 20–24, and 24–28 y) before diagnosis. n = 86,320 for 0–4 y, 84,071 for 4–8 y, 81,029 for 8–12 y, 77,200 for 12–16 y, 73,080 for 16–20 y, 67,780 for 20–24 y, and 61,722 for 24–28 y. CRC, colorectal cancer; DFE: dietary folate equivalent; NSAIDs, nonsteroidal anti-inflammatory drugs.