

Introduction
Lichen planus (LP) is a common inflammatory condition of the skin and mucous membranes with an uncertain etiology. Typical presentation sites for LP are the flexor surfaces, the trunk, as well as the oral or genital mucosa. The classic lesions have a well-established clinical appearance and histologic features, which aid in the diagnosis.1,2 Ocular LP is an extremely rare presentation most commonly affecting the eyelids, conjunctiva, and cornea and which can lead to severe scarring, with ocular LP being clinically indistinguishable from other causes of scarring.3, 4, 5, 6, 7
Case report
A 42-year-old woman presented with recurrent oral ulcerations, eye irritation, and redness (Fig 1) as well as facial pustules and erythema. There were no oral lesions at the time of presentation. Evaluation by ophthalmology was requested, and a diagnosis of ocular rosacea with blepharitis and dry eye was rendered. Tests for anti-nuclear, anti-SSA, and anti-SSB antibodies were all negative. The patient was found to be hypothyroid, and thyroid replacement therapy was started. A biopsy of the oral lesions had been previously performed by an oral surgeon, with reported pathology being nonspecific.
Fig 1.

Erythema of upper portion and lower portion of the eyelids.
The patient was treated with tobramycin/dexamethasone eye drops and baby shampoo eyelid scrubs from the ophthalmologist, with minimal improvement. The patient's rosacea improved with oral doxycycline 100 mg/day and topical azelaic acid; however, the sporadic oral lesions continued. With continued irritation of the eyelids, a biopsy of the eyelid was obtained for direct immunofluorescence, which excluded cicatricial pemphigoid. The biopsy (Fig 2) was consistent with LP. The previous biopsy slide from the oral lesion was obtained, and it also revealed LP.
Fig 2.
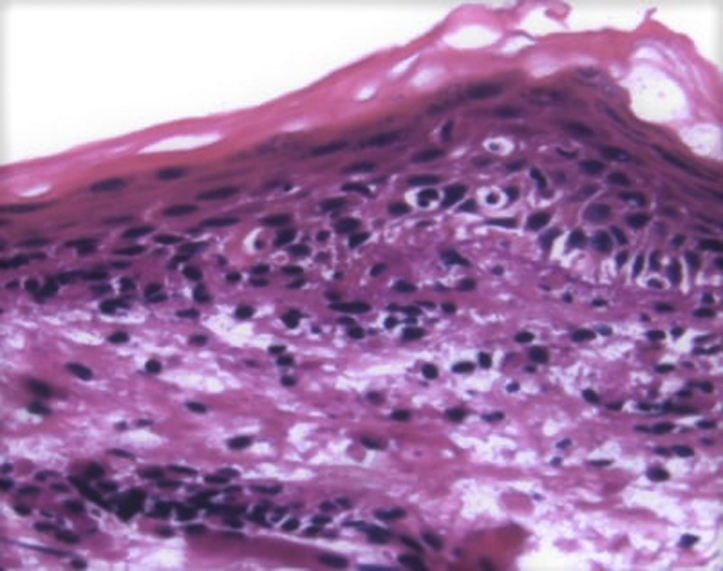
Punch biopsy of the upper portion of the right eyelid showed a lichenoid infiltrate of lymphocytes in the papillary dermis with infiltration of the epidermis. Associated basal cell layer vacuolar change was observed. A few dyskeratotic cells were noted within the epidermis. The granular layer was intact. Compact orthokeratosis was observed to overlie the epidermis without parakeratosis. (Hematoxylin-eosin staining of a frozen direct immunofluorescence slide, original magnification: ×400).
With the diagnosis of probable ocular LP, the patient was initiated on topical cyclosporine drops, and, after some time, exhibited minimal improvement. Given the concerns for continued ocular inflammation and the risk of loss of vision due to scarring, the patient was started on oral mycophenolate mofetil 500 mg 2 pills twice a day and experienced a quick resolution of her symptoms. After several months without symptoms, mycophenolate mofetil was slowly withdrawn, and the ocular symptoms returned. It was decided to recommence the mycophenolate mofetil and continue for a longer time prior to discontinuing the medication.
Discussion
Ocular LP is a rarely reported entity, with conjunctival LP reported in 19288 and LP of the eyelids in 1938.8, 9, 10, 11 It may occur in the form of pruritic violaceous papules of the eyelids, but, as in our case, may only present as irritation of the eye lids (Table I),10,12,13 blepharitis, and eventually, keratitis. A review of the literature revealed 22 previously reported cases of ocular LP, with this case bringing the total to 23. Of the reported cases, 19 out of 23 (83%) affected individuals of the female gender, and 6 out of 23 (26%) had only ocular involvement of their LP.14, 15, 16
Table I.
Common causes of eyelid dermatosis
| 1. Allergic dermatitis |
| 2. Atopic dermatitis |
| 3. Seborrheic dermatitis |
| 4. Xerosis |
| 5. Discoid lupus |
| 6. Dermatomyositis |
| 7. Psoriasis |
| 8. Lichen planus |
Ocular LP can involve the eyelids (Table I), but can also involve the conjunctiva and lacrimal structures. Ocular LP can lead to irreversible damage to the surface of the eye and loss of vision. Conjunctival involvement can lead to cicatrization and subepithelial scarring (Table II) with involvement of the lacrimal structures leading to dry eye. Ocular LP rarely responds to local ocular therapy.7,8,10
Table II.
Common causes of cicatricial conjunctivitis
|
|
|
|
Our patient had dryness, ocular inflammation, and eyelid irritation. Her oral lesions were later determined to be LP as well. As in many other reported cases, the diagnosis in our case was reached only after long-term topical treatment for severe blepharitis and eye irritation and continued search for a diagnosis.
Ocular LP of the eyelid or anterior segment of the eye is a rare entity and should be included in the differential diagnosis of eyelid dermatoses as well as blepharitis, keratitis, and conjunctivitis. Table I reviews common causes of eyelid dermatitis and Table II reviews common causes of cicatricial conjunctivitis. External causes of lichenoid reactions include medications, viral infections, and vaccines, none of which could be attributed to our patient's ocular LP.17 The majority of patients reported to date were of the female gender, and most did not have isolated lesions. Our patient did not respond well to topical agents, and we report the effective use of mycophenolate mofetil in this chronic condition in an effort to avoid potentially serious complications. More work needs to be done to elucidate the most appropriate therapies.
Conflicts of interest
None declared.
Footnotes
Funding sources: None.
IRB approval status: Not applicable.
References
- 1.Krupaa R.J., Sankari S.L., Masthan K.M.K., Rajesh E. Oral lichen planus: an overview. J Pharm Bioallied Sci. 2015;7(suppl 1):S158–S161. doi: 10.4103/0975-7406.155873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Webster G.F., Durrani K., Suchecki J. Ocular rosacea, psoriasis, and lichen planus. Clin Dermatol. 2016;34(2):146–150. doi: 10.1016/j.clindermatol.2015.11.014. [DOI] [PubMed] [Google Scholar]
- 3.Nekolová J., Středová M., Podhola M., Jirásková N. Lichen planus as a possible rare cause of an ocular disease. Cesk Slov Oftalmol. 2019;75(4):219–223. doi: 10.31348/2019/4/6. [DOI] [PubMed] [Google Scholar]
- 4.Huang S., Channa P. Cicatricial keratoconjunctivitis associated with lichen planus. GMS Ophthalmol Cases. 2015;7(5):1–3. doi: 10.3205/oc000030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Igras E., Kennedy S., MacDermott E.J., Murphy C.C. Isolated ocular lichen planus in a child. J AAPOS. 2015;19(4):381–383. doi: 10.1016/j.jaapos.2015.03.019. [DOI] [PubMed] [Google Scholar]
- 6.Thorne J.E., Jabs D.A., Nikolskaia O.V., Mimouni D., Anhalt G.J., Nousari H.C. Lichen planus and cicatrizing conjunctivitis: characterization of five cases. Am J Ophthalmol. 2003;136(2):239–243. doi: 10.1016/s0002-9394(03)00147-8. [DOI] [PubMed] [Google Scholar]
- 7.Webber N.K., Setterfield J.F., Lewis F.M., Neill S.M. Lacrimal canlicular duct scarring in patients with lichen planus. Arch Dermatol. 2012;148(2):224–227. doi: 10.1001/archdermatol.2011.580. [DOI] [PubMed] [Google Scholar]
- 8.Michelson H.E., Laymon C. Lichen planus of the eyelids. Arch Dermatol. 1938;37(1):27–29. [Google Scholar]
- 9.Luhr A.F. Lichen planus of the conjunctiva. Am J Ophthalmol. 1924;7(6):456–457. [Google Scholar]
- 10.Rozas Muñoz E., Martínez-Escala M.E., Juanpere N., Armentia J., Pujol R.M., Herrero-Gonazáles J.E. Isolated conjunctival lichen planus. A diagnostic challenge. Arch Dermatol. 2011;147(4):465–467. doi: 10.1001/archdermatol.2011.68. [DOI] [PubMed] [Google Scholar]
- 11.Pakravan M., Klesert T.R., Akpek E.K. Isolated lichen planus of the conjunctiva. Br J Ophthalmol. 2006;90(10):1325–1326. doi: 10.1136/bjo.2006.096263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Verma S.B. Lichen planus affecting eyelid alone: a rare entity. Indian J Dermatol Venereol Leprol. 2006;72(5):398. doi: 10.4103/0378-6323.27771. [DOI] [PubMed] [Google Scholar]
- 13.Itin P.H., Buechner S.A., Rufli T. Lichen planus of the eyelids. Dermatology. 1995;191(4):350–351. doi: 10.1159/000246599. [DOI] [PubMed] [Google Scholar]
- 14.Bevans S.L., Theos A.J., Fowler P.G., Pavlidakey P.G., Stoll M., Sami N. Pediatric ocular lichen planus and lichen planopilaris: one new case and a review of the literature. Pediatr Dermatol. 2018;35(6):859–863. doi: 10.1111/pde.13606. [DOI] [PubMed] [Google Scholar]
- 15.Huang Y.Y.M., Wang C.M., Potenziani S., Hsu S. Lichen planus of the eyelids: a case report and review of the literature. Dermatol Online J. 2017;23(2) 13030/qt1c04h08s. [PubMed] [Google Scholar]
- 16.Ozlu E., Teberik K. Evaluation of ocular findings in patients with lichen planus. Postepy Dermatol Alergol. 2019;36(3):267–271. doi: 10.5114/ada.2018.74464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dyall-Smith D. Lichenoid drug eruption. 2010. https://dermnetnz.org/topics/lichenoid-drug-eruption/