
Fig. 2.
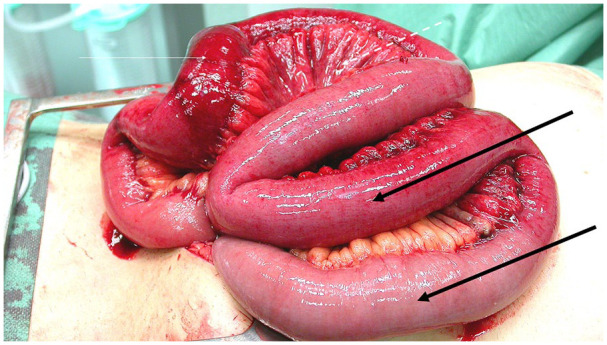
Explorative laparotomy in a patient with MVT. At laparotomy, 0.4 m of the most reddish and severely ischemic segment (thin arrow) was resected and anastomosed. Note the distended small bowel loops (thick black arrows) and the edema in the adjacent mesentery (dashed line). Histopathology of the resected bowel did not show transmural infarction but did show infarcted mucosa and venous thrombosis. It is uncertain whether bowel resection really was necessary or if the ischemic bowel would have recovered without bowel resection and anticoagulation therapy alone.