
Figure 2.
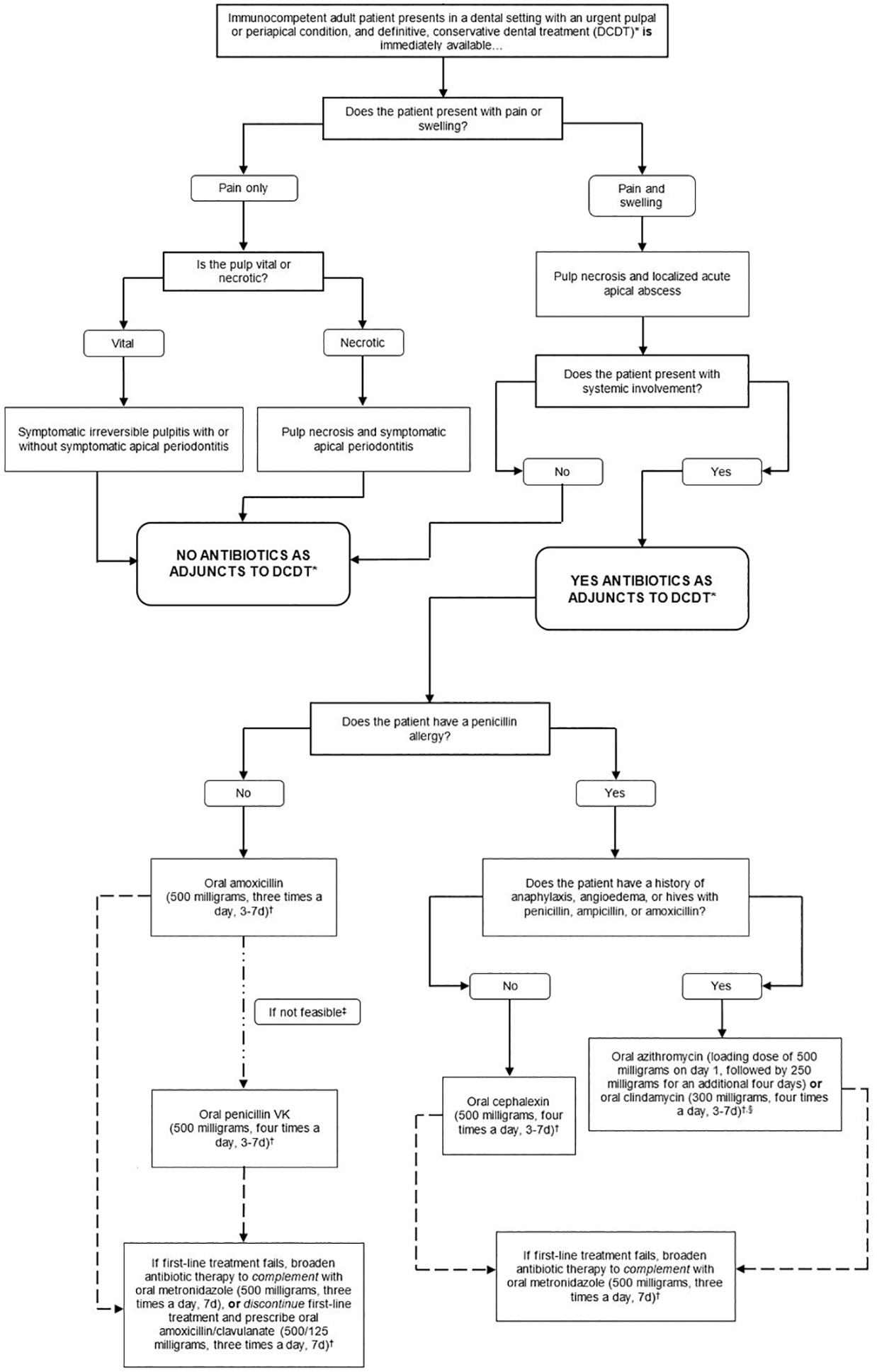
Clinical pathway for the treatment of immunocompetent adult patients presenting in a dental setting with a pulpal or periapical condition where treatment is immediately available
Footnotes
* Definitive, conservative dental treatment refers to pulpotomy, pulpectomy, non-surgical root canal treatment, or incision for drainage of abscess. Only clinicians who are authorized or trained to perform the specified treatments should do so.
† Clinicians should reevaluate patient within 3 days (e.g., in-person visit or phone call). Dentists should instruct patients to discontinue antibiotics 24 hours after patient’s symptoms resolve, irrespective of reevaluation after three days.
‡ Although the expert panel recommends both amoxicillin and penicillin as first-line treatments, amoxicillin is preferred over penicillin because it is more efficacious against various gram-negative anaerobes and its lower incidence of gastrointestinal side effects.
§ Bacterial resistance rates for azithromycin are higher than for other antibiotics, and clindamycin substantially increases the risk of Clostridioides difficile infection (CDI) even after a single dose (Thornhill. 2015). Due to concerns about antibiotic resistance, patients who receive azithromycin should be instructed to closely monitor their symptoms and call a dentist or primary care provider if their infection worsens while on therapy. Similarly, clindamycin has a U.S. Food and Drug Administration Black Box warning for CDI, which can be fatal. Patients should be instructed to call their primary care provider if they develop fever, abdominal cramping, or ≥3 loose bowel movements per day (Leffler, 2015). If the patient is currently taking an antibiotic within the same spectrum as the one indicated, additional antibiotics do not need to be prescribed. If the patient is currently taking an antibiotic outside of the spectrum as the one indicated, the intended antibiotic can still be prescribed, considering potential contraindications. An antibiotic with a similar spectrum of activity to those recommended can be continued if the antibiotic was initiated prior to patient presentation. As with any antibiotic use, the patient should be instructed on symptoms that may indicate lack of antibiotic efficacy and adverse drug events.