
FIGURE.
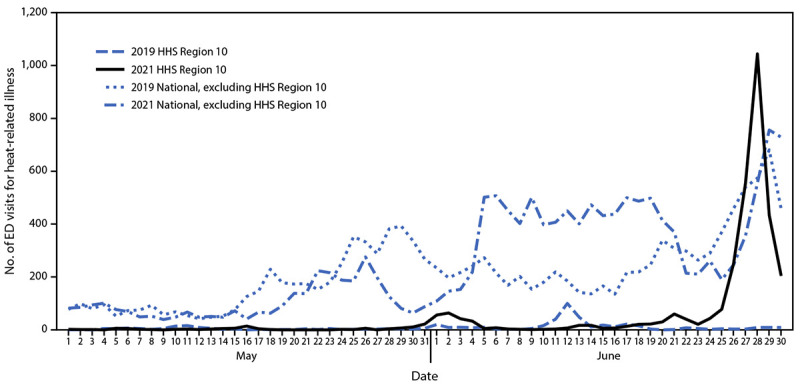
Number of emergency department visits for heat-related illness* in U.S. Department of Health and Human Services Region 10† and nationwide (excluding Region 10), by year§ — National Syndromic Surveillance Program,¶ United States, May 1–June 30, 2019 and May 1–June 30, 2021
Abbreviations: ED = emergency department; HHS = U.S. Department of Health and Human Services; NSSP = National Syndromic Surveillance Program.
* ED visits for heat-related illness were identified using a combination of free-text reason for visit (chief complaint) and discharge diagnosis codes indicating exposure to high ambient temperature.
† HHS Region 10 includes Alaska, Idaho, Oregon, and Washington.
§ To limit the effect of data quality on trends, all 2019–2021 comparison analyses were restricted to facilities with a coefficient of variation ≤40 and weekly average informative discharge diagnosis of ≥75% throughout the analysis period May 1–June 30, 2019 and May 1–June 30, 2021, so that only facilities with consistent reporting and more complete data were included. This helps account for changes over time in the number of facilities sharing data with NSSP, which can impact analyses involving multi-year comparisons.
¶ NSSP is a collaboration between CDC, local and state health departments, federal agencies, health care facilities, independent clinical laboratories, and a university-affiliated research center. NSSP receives data from 71% of nonfederal EDs nationwide, although <50% of ED facilities from California, Hawaii, Iowa, Ohio, Minnesota, and Oklahoma currently participate in NSSP. Among all visit data received by NSSP, 78% are reported within 24 hours of the clinical encounter. NSSP collects ED visit information (chief complaint and administrative discharge diagnosis) and patient demographic details such as age, gender, race, and ethnicity. Diagnosis information is collected using the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) and (ICD-9-CM), and Systematized Nomenclature of Medicine (SNOMED) codes.