

Abstract
Women with polycystic ovary syndrome (PCOS) have a substantially increased risk for diabetes and cardiovascular disease. Obstructive sleep apnea (OSA) is the most common sleep disorder in PCOS. Recent population-based studies indicate a high incidence of OSA among adult women with PCOS. Obesity and increasing age are the main factors for this association. There is strong evidence indicating that OSA is an important modulator of metabolic risk in the general population. There is also some evidence to suggest that OSA may contribute to insulin resistance and glucose intolerance among women PCOS, and thus increase their metabolic risk. The potential mechanisms for adverse metabolic consequences of OSA are likely to be multiple. Whether treatment of OSA in PCOS improves metabolic outcomes requires further rigorous research.
Keywords: PCOS, Obstructive sleep apnea, Glucose, Insulin resistance, Diabetes, Metabolic, Cardiovascular
Introduction
Polycystic ovary syndrome (PCOS) is the most common endocrine disorder in women of reproductive age. The syndrome was initially defined in the 1930s by reproductive abnormalities including oligomenorrhea, anovulation, and infertility [1]. Decades later, insulin resistance and related metabolic derangements were identified as key features in PCOS [2]. It is now well-established that affected women are at a high risk for early-onset diabetes and cardiovascular disease [3]. In addition, it is increasingly recognized that sleep disturbances, particularly obstructive sleep apnea (OSA) are highly prevalent in PCOS [4–6]. There is also some evidence to suggest that the presence and severity of OSA may worsen insulin resistance and glucose intolerance in this high-risk population [4,7,8].
OSA is characterized by recurring complete (i.e., apnea) or partial (i.e., hypopnea) upper airway obstruction leading to intermittent hypoxia (i.e., repetitive cycles of oxygen drops and reoxygenation), sleep fragmentation, and poor sleep quality. OSA is a treatable disorder that is pervasive in overweight and obese individuals [9]. Continuous positive airway pressure (CPAP) is the recommended first-line treatment for individuals who are diagnosed with OSA. However, it is estimated that, in the general population, about 80% of those who have OSA remain undiagnosed, and thus not receive CPAP treatment [9–11]. The gold standard for establishing OSA diagnosis is by polysomnography when the apnea-hypopnea index, that is, the total number of obstructive apneas and hypopneas per hour of sleep, is greater than five [12]. Typical symptoms of OSA include snoring, witnessed apneas, daytime sleepiness, and cognitive impairment. Clinically, women with OSA may often present with insomnia, fatigue, or mood disturbances, rather than snoring or daytime sleepiness. Obesity and increasing age are major risk factors for OSA. Also, men are more likely to have OSA than women [13]. Over the past 20 years, numerous studies have demonstrated that beyond the effects of excess weight, OSA may be an important determinant of insulin resistance and glucose intolerance, and thus may contribute to the development of diabetes and cardiovascular disease (reviewed in Refs. [14–16]). In lean individuals, OSA was associated with insulin resistance and higher glucose as compared to controls that were matched for BMI and visceral adiposity [17,18].
Herein, we review the current evidence for associations between OSA and PCOS with a particular focus on the impact of OSA on insulin resistance and glucose intolerance in affected women. We also briefly discuss the potential mechanisms by which OSA can result in metabolic dysfunction, and thus may contribute to heightened metabolic risk in PCOS.
Prevalence of OSA in PCOS: clinical and population-based studies
The associations between and OSA and PCOS were first identified in clinical studies reporting an increased prevalence of OSA, estimated on average at ~40%, among women with PCOS (reviewed in the study by Kahal et al. [19]). Notably, the clinical studies were limited by small sample size and inclusion of mostly overweight or obese women with PCOS [20–26]. A few studies also reported that this association was stronger particularly during rapid eye movement sleep [23,27], a sleep stage when predisposition to upper airway collapse is increased particularly in the presence of excess weight. In a recent meta-analysis of 12 clinical studies (8 in adults and 5 in adolescents) that used polysomnography [6], adult women with PCOS had a 9.7 times higher risk for OSA than control women of similar age. However, obesity was not accounted for in this meta-analysis and in most studies, PCOS women were heavier than controls. Furthermore, this association was not observed among adolescent girls, suggesting that increased age may be an important determinant of OSA in PCOS. More specifically, the prevalence of OSA was not increased in obese adolescents with PCOS compared with normal weight or obese girls without PCOS [28–30]. Nevertheless, abnormalities in sleep architecture with reduced sleep efficiency, reduced rapid eye movement sleep, and increased sleep latency were found among girls with PCOS compared with lean or obese controls [30]. In a retrospective chart review, the prevalence of OSA was increased in obese adolescents with PCOS compared with obese controls, with estimates similar to that reported in obese adolescent boys [31].
More recently, population-based studies have shown an association between PCOS and OSA [32,33] and other sleep disturbances, for example, difficulty initiating and maintaining sleep or insomnia [34–36]. These associations were not entirely explained by excess weight alone in these population-based longitudinal analyses. The high rates of insomnia symptoms in PCOS may reflect, at least in part, an unrecognized OSA diagnosis, because women frequently present with OSA with atypical symptoms [37]. In a longitudinal analysis of the large Taiwan National Health Insurance Research Database, using formal diagnosis codes women with PCOS (n = 4595) had greater incidence of OSA during a 2- to 8-year follow-up period, compared with age-matched control women, after adjusting for obesity, other demographics, and comorbidities (adjusted hazard ratio 2.6, 95% confidence interval 1.6–4.0) [32]. Similarly, another large population–based study from the UK, The Health Improvement Network, reported higher incidence of OSA in women with PCOS (n = 76 978) over a median follow-up of 3.5 years, as compared with age- and weight-matched women without PCOS (n = 143 077; adjusted hazard ratio 2.3, 95% confidence interval 1.9–2.7) [33]. In the UK cohort, the increased risk of OSA in PCOS was evident among overweight or obese women, but this association did not reach statistical significance in the normal weight group. Potential mechanisms other than obesity that might increase the likelihood of OSA in PCOS may involve intrinsic features such as central adiposity, hyperandrogenism, low progesterone, and low estradiol levels, which all have been implicated in OSA pathophysiology [7,38]. Hyperandrogenism, a cardinal feature of PCOS [39] can predispose to OSA via effects on neural control of breathing [40] and upper airway mechanics [41]. High androgen levels in PCOS have been associated with increased risk for OSA in some [20,26,42] but not all studies [24]. In addition, low progesterone and low estrogen concentrations can possibly contribute to this risk because low levels might increase frequency of apneic events in women across a broad age spectrum [43,44].
In summary, clinical studies suggest that the prevalence of OSA is increased in women with PCOS, but this association occurs in later life and appears to be mostly dependent on excess weight. Recent large population–based reports indicate a higher incidence of OSA in PCOS, which is not merely accounted for by obesity. Future rigorous research is necessary to elucidate the putative role of altered sex steroid production in elevated OSA risk seen in PCOS.
Impact of OSA on insulin resistance and glucose intolerance in PCOS
A few clinical studies have investigated the effects of OSA on metabolic outcomes in PCOS. In an earlier study, women with PCOS who were recommended treatment for OSA showed higher fasting insulin levels and a lower glucose-to-insulin ratio as compared with control women, and the difference between the insulin levels remained significant after adjustment for BMI [27]. More recent studies reported significant associations between the presence of OSA and fasting glucose [26] or insulin resistance by homeostatic model assessment (HOMA) index [42] among women with PCOS, after statistical adjustments for BMI. Similarly, among adolescent girls with PCOS and OSA, the degree of insulin resistance (HOMA index) was higher compared to girls with PCOS without OSA [31]. In an earlier study, we have reported that the risk and severity of OSA (respiratory events and oxygen desaturations) are highly correlated with insulin levels and measures of glucose tolerance [23]. Among women with normal glucose tolerance, the insulin response to an oral glucose challenge was more than two-fold greater in those at high risk for OSA per Berlin Questionnaire, as compared with those at low risk [23]. In a follow-up study, we have found that the presence and severity of OSA predicts insulin resistance and glucose intolerance in nondiabetic women with PCOS, after controlling for age, BMI, and ethnicity [24]. The increasing apnea-hypopnea index was a significant predictor of fasting glucose and insulin, HOMA index as well as 2-h glucose levels during an oral glucose challenge. Interestingly, among PCOS women with normal glucose tolerance, the presence of OSA was associated with a nearly 2-fold higher fasting insulin level and HOMA index [24]. To date, in the only interventional study involving women with PCOS and OSA, our group has found that 8 weeks of CPAP treatment of OSA in young and morbidly obese PCOS women improves metabolic and cardiovascular outcomes [45]. Among women who were compliant with CPAP treatment (average use ~ 6.6 h per night), we found a modest improvement in insulin sensitivity as assessed by intravenous glucose tolerance test, after controlling for BMI. In addition, in this cohort, we observed reductions in markers of sympathetic activity (i.e., plasma norepinephrine and heart rate variability) and diastolic blood pressure after OSA treatment [45]. These beneficial effects were of greater magnitude with longer hours of CPAP use and of lesser magnitude in those with higher degrees of obesity. The potential mechanisms by which OSA may worsen metabolic outcomes could be multiple [46–48]. Intermittent hypoxia and sleep fragmentation can lead to metabolic disturbances via an interplay of intermediate pathways (Fig. 1) including sympathetic activation [49], alterations in lipid metabolism [50,51], oxidative stress and mitochondrial dysfunction [52], release of proinflammatory markers [53,54], and endothelial dysfunction [55,56]. In fact, the animal and human models mimicking OSA provide strong evidence to support these putative pathways. These models utilized experimental exposures to intermittent hypoxia and sleep fragmentation and revealed direct mechanistic links between OSA, insulin resistance, glucose intolerance, and beta-cell dysfunction [57–65].
Figure 1. Potential mechanisms linking OSA to adverse metabolic consequences.
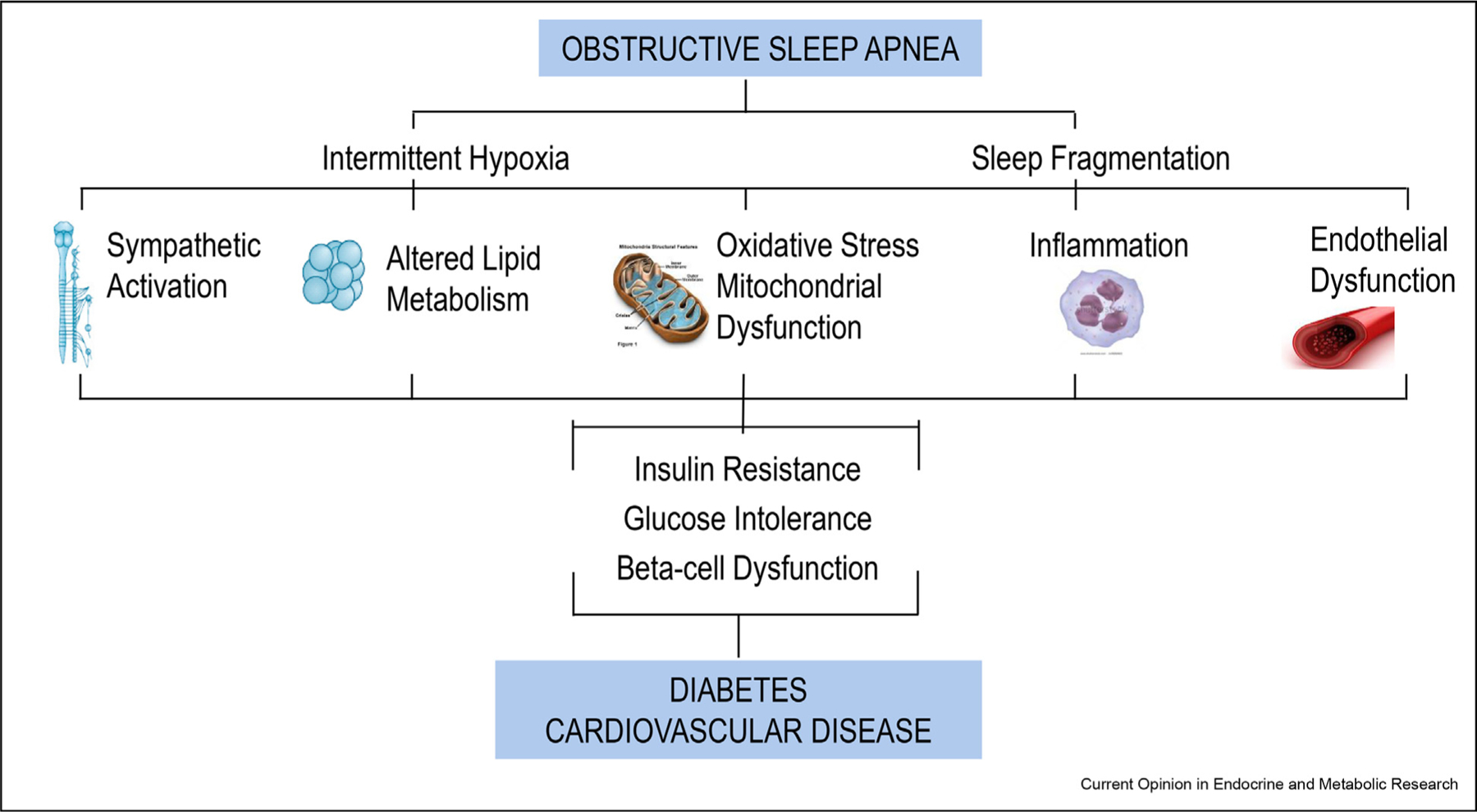
Intermittent hypoxia and sleep fragmentation are two main characteristics of OSA, which can result in sympathetic overactivity, alterations and lipid metabolism, oxidative stress and mitochondrial dysfunction, inflammation, and endothelial dysfunction. These metabolic disturbances may subsequently contribute to insulin resistance, glucose intolerance and beta-cell dysfunction, leading to diabetes, and cardiovascular disease.
Overall, a limited number of clinical studies suggest that the presence of OSA may exacerbate the degree of insulin resistance and glucose intolerance in PCOS, after statistical adjustments for BMI. It is noteworthy that these findings should be interpreted with caution considering small number of patients and higher degree of obesity among women with PCOS and OSA. Thus, the potential role of OSA in worsening metabolic risk in PCOS needs to be further investigated. Nevertheless, the current evidence in OSA populations without PCOS and experimental models mimicking OSA strongly supports a biological plausibility linking OSA to metabolic disturbances seen in PCOS.
Summary and future research agenda
OSA is a highly common sleep disorder particularly among overweight or obese populations. Yet, it is often overlooked and undertreated. Current evidence from clinical and population-based studies indicate that OSA occurs at increasing frequency among women with PCOS. Age and obesity appear to be major determinants in this association. In addition, observational evidence in a limited number of studies suggests that metabolic outcomes are worsened among PCOS women who have OSA. Numerous studies support a strong biological plausibility that OSA may be an important modulator of metabolic risk. Current guidelines recommend screening overweight or obese adolescents and adult women with PCOS for symptoms suggestive of OSA and to provide appropriate treatment if OSA is diagnosed [66]. The question of whether the presence of OSA may exacerbate the metabolic risk in PCOS requires further rigorous research to better understand the underlying pathophysiology. Large-scale randomized controlled trials of CPAP treatment of OSA with robust assessments of insulin sensitivity and glucose tolerance of are also warranted. In addition, future mechanistic studies can provide novel pathophysiologic insights to the associations between OSA and heightened metabolic risk in PCOS.
Funding declaration
Dr.Tasali’s research is funded by R01 DK120312-01A1 and R01DK115471 from the National Institute of Health.
Footnotes
Conflict of interest statement
Nothing declared.
References
Papers of particular interest, published within the period of review, have been highlighted as:
* of special interest
** of outstanding interest
- 1.Stein IF LM: Amenorrhea associated with bilateral polycystic ovaries. Am J Obstet Gynecol 1935, 29:181–191. [Google Scholar]
- 2.Dunaif A, Segal KR, Shelley DR, Green G, Dobrjansky A, Licholai T: Evidence for distinctive and intrinsic defects in insulin action in polycystic ovary syndrome. Diabetes 1992, 41:1257–1266. [DOI] [PubMed] [Google Scholar]
- 3.Osibogun O, Ogunmoroti O, Michos ED: Polycystic ovary syndrome and cardiometabolic risk: opportunities for cardiovascular disease prevention. Trends Cardiovasc Med 2020, 30: 399–404. [DOI] [PubMed] [Google Scholar]
- 4.**.Sam S, Ehrmann DA: Pathogenesis and consequences of disordered sleep in PCOS. Clin Med Insights Reprod Health 2019, 13. 1179558119871269. [DOI] [PMC free article] [PubMed] [Google Scholar]; This review article provides an excellent overview of the pathogenesis of obstructive sleep apnea in PCOS and its association with metabolic disorders.
- 5.Fernandez RC, Moore VM, Van Ryswyk EM, Varcoe TJ, Rodgers RJ, March WA, Moran LJ, Avery JC, McEvoy RD, Davies MJ: Sleep disturbances in women with polycystic ovary syndrome: prevalence, pathophysiology, impact and management strategies. Nat Sci Sleep 2018, 10:45–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.*.Helvaci N, Karabulut E, Demir AU, Yildiz BO: Polycystic ovary syndrome and the risk of obstructive sleep apnea: a meta-analysis and review of the literature. Endocr Connect 2017, 6: 437–445. [DOI] [PMC free article] [PubMed] [Google Scholar]; This is a meta-analysis of clinical studies that utilized overnight polysomnography to examine the association between PCOS and the occurrence of OSA with a particular focus on the effects of obesity, insulin resistance and androgen excess on this association
- 7.*.Tasali E, Van Cauter E, Ehrmann DA: Polycystic ovary syndrome and obstructive sleep apnea. Sleep Med Clin 2008, 3: 37–46. [DOI] [PMC free article] [PubMed] [Google Scholar]; This article provides a summary of potential pathophysiological links between PCOS and obstructive sleep apnea. The pathogenesis of cardiometabolic abnormalities in PCOS, the putative role of sex steroids in promoting OSA among PCOS women, and the potential effects of OSA in the increased metabolic risk in PCOS are discussed.
- 8.*.Kahal H, Kyrou I, Uthman O, Brown A, Johnson S, Wall P, Metcalfe A, Tahrani AA, Randeva HS: The association between obstructive sleep apnea and metabolic abnormalities in women with polycystic ovary syndrome: a systematic review and meta-analysis. Sleep 2018, 41. [DOI] [PubMed] [Google Scholar]; This is a sytematic review of clinical studies that compared PCOS women with OSA to those without OSA to assesss health outcomes in affected women
- 9.Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM: Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol 2013, 177:1006–1014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Watson NF: Health care savings: the economic value of diagnostic and therapeutic care for obstructive sleep apnea. J Clin Sleep Med 2016, 12:1075–1077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Frost, Sullivan: Hidden health crisis costing America billions: underdiagnosing and undertreating obstructive sleep apnea draining healthcare system. Am Acad Sleep Med 2016. Available from: http://www.aasmnet.org/sleep-apnea-economic-impact. aspx; 2016 (Darien, IL.). [Google Scholar]
- 12.Epstein LJ, Kristo D, Strollo PJ Jr, Friedman N, Malhotra A, Patil SP, Ramar K, Rogers R, Schwab RJ, Weaver EM, Weinstein MD: Adult obstructive sleep apnea task force of the American academy of sleep, clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med 2009, 5:263–276. [PMC free article] [PubMed] [Google Scholar]
- 13.Punjabi NM: The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc 2008, 5:136–143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Punjabi NM, Beamer BA: Alterations in glucose disposal in sleep-disordered breathing. Am J Respir Crit Care Med 2009, 179:235–240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.**.Pamidi S, Aronsohn RS, Tasali E: Obstructive sleep apnea: role in the risk and severity of diabetes. Best Pract Res Clin Endocrinol Metabol 2010, 24:703–715. [DOI] [PMC free article] [PubMed] [Google Scholar]; This is an excellent review of numerous epidemiologic, clinical and experimental studies linking OSA to alterations in glucose metabolism in various populations.
- 16.Kent BD, McNicholas WT, Ryan S: Insulin resistance, glucose intolerance and diabetes mellitus in obstructive sleep apnoea. J Thorac Dis 2015, 7:1343–1357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Pamidi S, Wroblewski K, Broussard J, Day A, Hanlon EC, Abraham V, Tasali E: Obstructive sleep apnea in young lean men: impact on insulin sensitivity and secretion. Diabetes Care 2012, 35:2384–2389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lin QC ZX, Chen GP, Huang DY, Din HB, Tang AZ: Obstructive sleep apnea syndrome is associated with some components of metabolic syndrome in nonobese adults. Sleep Breath 2011. [DOI] [PubMed] [Google Scholar]
- 19.Kahal H, Kyrou I, Tahrani AA, Randeva HS: Obstructive sleep apnoea and polycystic ovary syndrome: a comprehensive review of clinical interactions and underlying pathophysiology. Clin Endocrinol 2017, 87:313–319. [DOI] [PubMed] [Google Scholar]
- 20.Fogel RB, Malhotra A, Pillar G, Pittman SD, Dunaif A, White DP: Increased prevalence of obstructive sleep apnea syndrome in obese women with polycystic ovary syndrome. J Clin Endocrinol Metab 2001, 86:1175–1180. [DOI] [PubMed] [Google Scholar]
- 21.Gopal M, Duntley S, Uhles M, Attarian H: The role of obesity in the increased prevalence of obstructive sleep apnea syndrome in patients with polycystic ovarian syndrome. Sleep Med 2002, 3:401–404. [DOI] [PubMed] [Google Scholar]
- 22.Vgontzas AN, Legro RS, Bixler EO, Grayev A, Kales A, Chrousos GP: Polycystic ovary syndrome is associated with obstructive sleep apnea and daytime sleepiness: role of insulin resistance. J Clin Endocrinol Metabol 2001, 86:517–520. [DOI] [PubMed] [Google Scholar]
- 23.Tasali E, Van Cauter E, Ehrmann DA: Relationships between sleep disordered breathing and glucose metabolism in polycystic ovary syndrome. J Clin Endocrinol Metab 2006, 91: 36–42. [DOI] [PubMed] [Google Scholar]
- 24.**.Tasali E, Van Cauter E, Hoffman L, Ehrmann DA: Impact of obstructive sleep apnea on insulin resistance and glucose tolerance in women with polycystic ovary syndrome. J Clin Endocrinol Metab 2008, 93:3878–3884. [DOI] [PMC free article] [PubMed] [Google Scholar]; This is a clinical study comparing metabolic outcomes among nondiabetic PCOS women with and without OSA, and control women. The findings showed that OSA is an important determinant of insulin resistance and glucose intolerance in PCOS
- 25.Mokhlesi B, Scoccia B, Mazzone T, Sam S: Risk of obstructive sleep apnea in obese and nonobese women with polycystic ovary syndrome and healthy reproductively normal women. Fertil Steril 2012, 97:786–791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chatterjee B, Suri J, Suri JC, Mittal P, Adhikari T: Impact of sleep-disordered breathing on metabolic dysfunctions in patients with polycystic ovary syndrome. Sleep Med 2014, 15: 1547–1553. [DOI] [PubMed] [Google Scholar]
- 27.Vgontzas AN, Legro RS, Bixler EO, Grayev A, Kales A, Chrousos GP: Polycystic ovary syndrome is associated with obstructive sleep apnea and daytime sleepiness: role of insulin resistance. J Clin Endocrinol Metabol 2001, 86:517–520. [DOI] [PubMed] [Google Scholar]
- 28.de Sousa G, Schluter B, Buschatz D, Menke T, Trowitzsch E, Andler W, Reinehr T: A comparison of polysomnographic variables between obese adolescents with polycystic ovarian syndrome and healthy, normal-weight and obese adolescents. Sleep Breath 2010, 14:33–38. [DOI] [PubMed] [Google Scholar]
- 29.de Sousa G, Schluter B, Menke T, Trowitzsch E, Andler W, Reinehr T: Relationships between polysomnographic variables, parameters of glucose metabolism, and serum androgens in obese adolescents with polycystic ovarian syndrome. J Sleep Res 2011, 20:472–478. [DOI] [PubMed] [Google Scholar]
- 30.de Sousa G, Schluter B, Buschatz D, Menke T, Trowitzsch E, Andler W, Reinehr T: The impact of insulin resistance and hyperandrogenemia on polysomnographic variables in obese adolescents with polycystic ovarian syndrome. Sleep Breath 2012, 16:169–175. [DOI] [PubMed] [Google Scholar]
- 31.Nandalike K, Agarwal C, Strauss T, Coupey SM, Isasi CR, Sin S, Arens R: Sleep and cardiometabolic function in obese adolescent girls with polycystic ovary syndrome. Sleep Med 2012, 13:1307–1312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lin TY, Lin PY, Su TP, Li CT, Lin WC, Chang WH, Chen TJ, Bai YM, Chen MH: Risk of developing obstructive sleep apnea among women with polycystic ovarian syndrome: a nationwide longitudinal follow-up study. Sleep Med 2017, 36: 165–169. [DOI] [PubMed] [Google Scholar]
- 33.*.Kumarendran B, Sumilo D, O’Reilly MW, Toulis KA, Gokhale KM, Wijeyaratne CN, Coomarasamy A, Arlt W, Tahrani AA, Nirantharakumar K: Increased risk of obstructive sleep apnoea in women with polycystic ovary syndrome: a population-based cohort study. Eur J Endocrinol 2019, 180:265–272. [DOI] [PMC free article] [PubMed] [Google Scholar]; This is the largest population-based analysis to date, reporting that beyond the effects of obesity, the incidence of OSA is increased in women with PCOS compared to control women.
- 34.Hung JH, Hu LY, Tsai SJ, Yang AC, Huang MW, Chen PM, Wang SL, Lu T, Shen CC: Risk of psychiatric disorders following polycystic ovary syndrome: a nationwide population-based cohort study. PloS One 2014, 9, e97041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Moran LJ, March WA, Whitrow MJ, Giles LC, Davies MJ, Moore VM: Sleep disturbances in a community-based sample of women with polycystic ovary syndrome. Hum Reprod 2015, 30:466–472. [DOI] [PubMed] [Google Scholar]
- 36.Mo L, Mansfield DR, Joham A, Cain SW, Bennett C, Blumfield M, Teede H, Moran LJ: Sleep disturbances in women with and without polycystic ovary syndrome in an Australian National Cohort. Clin Endocrinol 2019, 90:570–578. [DOI] [PubMed] [Google Scholar]
- 37.Theorell-Haglow J, Miller CB, Bartlett DJ, Yee BJ, Openshaw HD, Grunstein RR: Gender differences in obstructive sleep apnoea, insomnia and restless legs syndrome in adults - what do we know? A clinical update. Sleep Med Rev 2018, 38: 28–38. [DOI] [PubMed] [Google Scholar]
- 38.Eckert DJ, Malhotra A: Pathophysiology of adult obstructive sleep apnea. Proc Am Thorac Soc 2008, 5:144–153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Abbott DH, Dumesic DA, Levine JE: Hyperandrogenic origins of polycystic ovary syndrome - implications for pathophysiology and therapy. Expet Rev Endocrinol Metabol 2019, 14: 131–143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.White DP, Schneider BK, Santen RJ, McDermott M, Pickett CK, Zwillich CW, Weil JV: Influence of testosterone on ventilation and chemosensitivity in male subjects. J Appl Physiol 1985, 59:1452–1457. [DOI] [PubMed] [Google Scholar]
- 41.Cistulli PA, Grunstein RR, Sullivan CE: Effect of testosterone administration on upper airway collapsibility during sleep. Am J Respir Crit Care Med 1994, 149(2 Pt 1):530–532. [DOI] [PubMed] [Google Scholar]
- 42.Tock L, Carneiro G, Togeiro SM, Hachul H, Pereira AZ, Tufik S, Zanella MT: Obstructive sleep apnea predisposes to nonalcoholic Fatty liver disease in patients with polycystic ovary syndrome. Endocr Pract 2014, 20:244–251. [DOI] [PubMed] [Google Scholar]
- 43.Netzer NC, Eliasson AH, Strohl KP: Women with sleep apnea have lower levels of sex hormones. Sleep Breath 2003, 7: 25–29. [DOI] [PubMed] [Google Scholar]
- 44.Popovic RM, White DP: Upper airway muscle activity in normal women: influence of hormonal status. J Appl Physiol 1985, 84: 1055–1062. 1998. [DOI] [PubMed] [Google Scholar]
- 45.Tasali E, Chapotot F, Leproult R, Whitmore H, Ehrmann DA: Treatment of obstructive sleep apnea improves cardiometabolic function in young obese women with polycystic ovary syndrome. J Clin Endocrinol Metab 2011, 96:365–374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Mesarwi OA, Sharma EV, Jun JC, Polotsky VY: Metabolic dysfunction in obstructive sleep apnea: a critical examination of underlying mechanisms. Sleep Biol Rhythm 2015, 13:2–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Drager LF, Jun JC, Polotsky VY: Metabolic consequences of intermittent hypoxia: relevance to obstructive sleep apnea. Best Pract Res Clin Endocrinol Metabol 2010, 24:843–851. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Jun J, Polotsky VY: Metabolic consequences of sleep-disordered breathing. ILAR J 2009, 50:289–306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Somers VK, Dyken ME, Clary MP, Abboud FM: Sympathetic neural mechanisms in obstructive sleep apnea. J Clin Invest 1995, 96:1897–1904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ali AH, Mundi M, Koutsari C, Bernlohr DA, Jensen MD: Adipose tissue free fatty acid storage in vivo: effects of insulin versus niacin as a control for suppression of lipolysis. Diabetes 2015, 64:2828–2835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Chopra S, Rathore A, Younas H, Pham LV, Gu C, Beselman A, Kim IY, Wolfe RR, Perin J, Polotsky VY, Jun JC: Obstructive sleep apnea dynamically increases nocturnal plasma free fatty acids, glucose, and cortisol during sleep. J Clin Endocrinol Metab 2017, 102:3172–3181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Dewan NA, Nieto FJ, Somers VK: Intermittent hypoxemia and OSA: implications for comorbidities. Chest 2015, 147: 266–274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Ryan S: Adipose tissue inflammation by intermittent hypoxia: mechanistic link between obstructive sleep apnoea and metabolic dysfunction. J Physiol 2017, 595:2423–2430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Murphy AM, Thomas A, Crinion SJ, Kent BD, Tambuwala MM, Fabre A, Pepin JL, Roche HM, Arnaud C, Ryan S: Intermittent hypoxia in obstructive sleep apnoea mediates insulin resistance through adipose tissue inflammation. Eur Respir J 2017, 49. [DOI] [PubMed] [Google Scholar]
- 55.Jelic S, Lederer DJ, Adams T, Padeletti M, Colombo PC, Factor PH, Le Jemtel TH: Vascular inflammation in obesity and sleep apnea. Circulation 2010, 121:1014–1021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Hoyos CM, Melehan KL, Liu PY, Grunstein RR, Phillips CL: Does obstructive sleep apnea cause endothelial dysfunction? A critical review of the literature. Sleep Med Rev 2015, 20:15–26. [DOI] [PubMed] [Google Scholar]
- 57.Polak J, Shimoda LA, Drager LF, Undem C, McHugh H, Polotsky VY, Punjabi NM: Intermittent hypoxia impairs glucose homeostasis in C57BL6/J mice: partial improvement with cessation of the exposure. Sleep 2013, 36:1483–1490. 1490A-1490B. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Shin MK, Yao Q, Jun JC, Bevans-Fonti S, Yoo DY, Han W, Mesarwi O, Richardson R, Fu YY, Pasricha PJ, Schwartz AR, Shirahata M, Polotsky VY: Carotid body denervation prevents fasting hyperglycemia during chronic intermittent hypoxia. J Appl Physiol 1985, 117:765–776. 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Iiyori N, Alonso LC, Li J, Sanders MH, Garcia-Ocana A, O’Doherty RM, Polotsky VY, O’Donnell CP: Intermittent hypoxia causes insulin resistance in lean mice independent of autonomic activity. Am J Respir Crit Care Med 2007, 175:851–857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Polotsky VY, Li J, Punjabi NM, Rubin AE, Smith PL, Schwartz AR, O’Donnell CP: Intermittent hypoxia increases insulin resistance in genetically obese mice. J Physiol 2003, 552(Pt 1): 253–264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Yokoe T, Alonso LC, Romano LC, Rosa TC, O’Doherty RM, Garcia-Ocana A, Minoguchi K, O’Donnell CP: Intermittent hypoxia reverses the diurnal glucose rhythm and causes pancreatic beta-cell replication in mice. J Physiol 2008, 586: 899–911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Gharib SA, Khalyfa A, Abdelkarim A, Bhushan B, Gozal D: Integrative miRNA-mRNA profiling of adipose tissue unravels transcriptional circuits induced by sleep fragmentation. PloS One 2012, 7, e37669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Tasali E, Leproult R, Ehrmann DA, Van Cauter E: Slow-wave sleep and the risk of type 2 diabetes in humans. Proc Natl Acad Sci U S A 2008, 105:1044–1049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Stamatakis KA, Punjabi NM: Effects of sleep fragmentation on glucose metabolism in normal subjects. Chest 2010, 137: 95–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Wang N, Khan SA, Prabhakar NR, Nanduri J: Impairment of pancreatic beta-cell function by chronic intermittent hypoxia. Exp Physiol 2013, 98:1376–1385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Legro RS, Arslanian SA, Ehrmann DA, Hoeger KM, Murad MH, Pasquali R, Welt CK: Endocrine, Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2013, 98: 4565–4592. [DOI] [PMC free article] [PubMed] [Google Scholar]