

Abstract
BACKGROUND:
Meningococcal conjugate vaccines were licensed beginning in 2005 on the basis of serologic end points and recommended for use in adolescents. A single dose at age 11 to 12 years was expected to provide protection through late adolescence. We conducted a case-control evaluation of vaccine effectiveness (VE) and duration of protection of a meningococcal (groups A, C, W, and Y) polysaccharide diphtheria toxoid conjugate vaccine (MenACWY-D).
METHODS:
Cases of culture- or polymerase chain reaction-confirmed serogroup A, C, W, and Y meningococcal disease among adolescents were identified through meningococcal disease surveillance sites in the United States from January 1, 2006, through August 31, 2013. Attempts were made to enroll 4 friend and school controls per case. VE was calculated using the generalized estimating equation, controlling for underlying medical conditions and smoking.
RESULTS:
Serogroup C accounted for 88 (49%), serogroup Y 80 (44%), and serogroup W 13 (7%) of enrolled cases. Thirty-six (20%) cases and 87 (44%) controls received MenACWY-D. The overall VE estimate 0 to 8 years postvaccination was 69% (51% to 80%); VE was 79% (49% to 91%) at <1 year, 69% (44% to 83%) at 1 to <3 years, and 61% (25% to 79%) at 3 to <8 years. VE was 77% (57% to 88%) against serogroup C and 51% (1% to 76%) against serogroup Y.
CONCLUSIONS:
MenACWY-D was effective in the first year after vaccination but effectiveness waned 3 to <8 years postvaccination. The estimates of VE from this evaluation informed the Advisory Committee on Immunization Practices in its decision to add a booster dose of MenACWY.
Meningococcal disease incidence has been declining since the late 1990s, and during 2002-2011 there were ~600 to 1200 cases annually in the United States.1,2 In the absence of vaccination, adolescents have higher rates of disease and nasopharyngeal carriage compared with other age groups.3-6 Rates of meningococcal disease increase starting at 16 years of age and peak in late adolescence before declining to rates similar to other adult age groups. During 2002 to 2011, rates of meningococcal disease were lower in adolescents aged 11 to 15 years (0.1 to 0.2 cases/100 000 population) compared with adolescents aged 16 to 21 years (0.5 to 0.7 cases/100 000 population).1 Licensed in 2005, meningococcal (groups A, C, W, and Y) polysaccharide diphtheria toxoid conjugate vaccine, MenACWY-D (Menactra, Sanofi Pasteur, Swiftwater, PA), was the first of 2 meningococcal conjugate vaccines licensed and available for use in adolescents in the United States (package insert available at http://www.fda.gov/downloads//Vaccines/ApprovedProducts/UCM131170.pdf). Because of the relatively low incidence of meningococcal disease, prelicensure randomized controlled trials used evidence of serologic protection rather than clinical end points. An early estimate of MenACWY-D effectiveness by using a simulation approach was 80% to 85% in the first 3 years after vaccination.7 Because there is an increased incidence of meningococcal disease through late adolescence and vaccination is recommended at age 11 to 12 years, protection for 10 to 12 years is critical to a successful meningococcal vaccination program.
Meningococcal conjugate vaccine has been recommended for all US adolescents since 2005, but vaccination coverage increased slowly. During 2005–2007, because vaccine production was limited soon after licensure, vaccination recommendations focused on certain cohorts of adolescents, including 11- to 12-year-olds, those entering high school at 14 to 15 years of age, and college freshmen living in residence halls. These recommendations were expanded in 2007 to include all 11 through 18 year olds, preferably at 11 to 12 years of age, and in 2010 the Advisory Committee on Immunization Practices (ACIP) recommended a booster dose at age 16 years.
To evaluate the effectiveness of MenACWY-D against meningococcal disease, including duration of protection, we conducted a case-control evaluation in multiple US states. Meningococcal (groups A, C, W, and Y) oligosaccharide diphtheria CRM197 conjugate vaccine, MenACWY-CRM (Menveo, Novartis Vaccines, Siena, Italy), was licensed in 2010 and therefore was not included in this evaluation. We evaluated the effectiveness and duration of protection of a single dose of MenACWY-D.
METHODS
Evaluation Population
Cases of meningococcal disease were identified through Active Bacterial Core surveillance (ABCs) and MeningNet sites. ABCs is a population and laboratory based surveillance system coordinated by the Centers for Disease Control and Prevention (CDC) through the Emerging Infections Program.8 MeningNet sites were state and local health departments funded to conduct enhanced meningococcal disease surveillance through CDC Epidemiology and Laboratory Capacity cooperative agreements. Not all sites participated for the entire course of the evaluation (Supplemental Table 4). Through ABCs, ~13% of the US population was under surveillance. Depending on the year and the number of MeningNet sites participating, an additional 30% to 45% of the US population was under surveillance for this evaluation, for a total of 43% to 58% of the US population under surveillance through ABCs and MeningNet.
Case Identification
Meningococcal disease is a nationally reportable condition, and all cases require public health investigation, including investigation of the case’s close contacts. A standardized case report form was used that included information on onset date, hospitalization, and underlying medical conditions. Eligible cases were adolescents living in a surveillance area and ≥11 years of age and born on or after January 1, 1986, at the time of illness. The upper age of eligibility increased each year of the study to include adolescents who were recommended for vaccination in previous years of the study. The upper age limit in 2006 was ≤18 years, in 2007 was ≤19 years, etc). Cases were enrolled from January 1, 2006, through August 31, 2013. Cases of meningococcal disease were defined as those from which Neisseria meningitidis was isolated from a normally sterile body site or where N meningitidis DNA was detected by polymerase chain reaction (PCR) from a blood or cerebrospinal fluid specimen. Only cases with disease caused by a vaccine serogroup were eligible for the evaluation. There were no serogroup A cases during the evaluation time period.
Laboratory Identification
Meningococcal isolates were serogrouped at the state or local health department laboratory by using slide agglutination. Isolates were sent to the CDC for confirmation of serogroup by slide agglutination and PCR. In suspect cases that were culture negative, specimens including blood and/or cerebrospinal fluid were either sent to the state or local health department laboratory or the CDC for PCR testing. If N meningitidis DNA was detected by PCR at a health department laboratory, confirmatory PCR testing was done at the CDC.9
Enrollment
Evaluation personnel used a standard protocol to enroll cases with information collected from the case investigation. Up to 15 attempts were made to contact case patients by telephone on different days and at various times; mobile telephone numbers were used if provided as part of the case investigation. For adolescents <18 years of age, consent was obtained from the parent as well as assent from the minor adolescent. Case patients or the parents who gave oral informed consent were enrolled; written consent was obtained after the interview to obtain provider records of immunization history. Case patients were asked for names of friends for control enrollment, and consent to contact the named friends by the evaluation personnel. Due to difficulties enrolling friend controls, sites were asked to additionally enroll controls through the school that the case attended with consent from the case. Controls were eligible for enrollment if they were within 2 years of age of the case and lived in the state or surveillance site at the time of illness onset of the case. Consent and enrollment procedures for controls were the same as for cases. Attempts were made to enroll 4 controls per case.
Evaluation personnel interviewed cases and controls by telephone to obtain demographic characteristics, history of meningococcal vaccination, and information on underlying medical conditions that are associated with an increased risk for meningococcal disease. Information on social and behavioral characteristics, such as smoking tobacco, was also obtained. Questions about social history and recent medical illness were asked about for the month before the onset date of meningococcal disease in the matched case. For adolescents <18 years of age, questions were asked to the parent or guardian of the case or control. For cases who died as a result of meningococcal disease, a proxy such as a parent was interviewed. Subjects were also asked to provide information on health care providers or other places where they might have received vaccines. Evaluation personnel contacted these providers or used the state electronic immunization registry to obtain information on receipt of meningococcal vaccine, including date of vaccination, vaccine type, and lot number. Vaccine brand was confirmed by using lot numbers when available. Because information on vaccine product was required, cases and controls were considered vaccinated only if the vaccination record could be verified.
Statistical Analysis
Data were collated and entered into a Microsoft Access database (Microsoft, Redmond, WA) at the CDC. Analyses were done with SAS statistical software (version 9.3; SAS Institute, Inc, Cary, NC). We used data from the case report forms and χ2 analysis to compare characteristics of adolescents who were enrolled with those who were not. For both cases and controls, a dose of vaccine was determined to be valid if it had been received at least 10 days before onset of illness in the case. Cases and controls who reported no history of vaccination and for whom vaccination status could not be verified were considered to be unvaccinated. Cases and controls with history of meningococcal polysaccharide vaccination (n = 12) or a history of 2 doses of MenACWY-D (n = 5) were excluded from the analysis. One case received a dose of MenACWY-CRM and was excluded from the analysis; no controls received MenACWY-CRM. Underlying medical conditions were defined as 1 or more of the following: cancer, complement disorder, other immune deficiency disorder, diabetes mellitus, kidney disease, sickle cell disease, and asplenia.
We used the generalized estimating equation (GEE) to estimate vaccine effectiveness (VE). GEE models incorporate data from concordant case patient/control sets and from case patients with no matched controls. GEE models the correlation among members of clusters to calculate the odds of being a case among vaccinated and unvaccinated subjects.10 The presence of underlying medical conditions and smoking were controlled for in the model. Conditional logistic regression models were also performed with similar results, which are presented in Supplemental Table 5.
Human Subjects
The evaluation was determined to be public health program evaluation by the National Center for Immunization and Respiratory Diseases at the CDC in 2006. Alabama, Arizona, California (ABCs), Colorado, Connecticut, Florida, Georgia, Houston, Indiana, Kansas, Maryland, Massachusetts, Minnesota, Mississippi, New Mexico, North Carolina, New York, New York City, Oklahoma, Oregon, Philadelphia, Texas, and Washington were approved by their local institutional review board to participate in the evaluation; all other sites determined the evaluation to be public health program evaluation or relied on the CDC’s determination.
RESULTS
We identified 320 adolescents with serogroup C, W, or Y meningococcal disease during January 1, 2006, through August 31, 2013, in the participating sites. Of these cases, 181 (57%) were enrolled. According to the data from the case report form, enrolled cases were similar in demographic characteristics to unenrolled cases (Table 1). A total of 199 controls were enrolled; 1 or more control was matched to 88 (49%) of enrolled case patients. Among the enrolled controls, 153 (82%) were friend controls and 31 (17%) were school controls. Case and control enrollment by year is shown in Table 1. Cases were less likely than controls to be white (67% vs 85%), were more likely to report an underlying medical condition (12% vs 2%), and to smoke (34% vs 25%). Underlying conditions for controls included cancer (n = 1), diabetes (n = 1), and other immunodeficiency disorder, not specified (n = 2). Underlying conditions for cases included cancer (n = 2), complement deficiency (n = 5), diabetes (n = 3), kidney disease (n = 2), asplenia (n = 1), and other immunodeficiency disorder, not specified (n = 9).
TABLE 1.
Characteristics of Eligible and Enrolled Cases-Patients, and Controls, ABCs and MeningNet Sites, 2006 to 2013
| Eligible Cases, n = 320 | Enrolled Cases, n = 181 | Controls, n = 199 | |
|---|---|---|---|
| Mean age, y | 18.9 (11 to 27) | 19.2 (11 to 27) | 18.9 (12 to 25) |
| Men, n (%) | 184 (58) | 107 (59) | 102 (51) |
| Race, n (%) | |||
| White | 213 (67) | 121 (67) | 170 (85) |
| African American | 64 (20) | 36 (20) | 10 (5) |
| Other | 14 (4) | 8 (4) | 15 (8) |
| Reported smoker, n (%) | — | 62 (34) | 49 (25) |
| Reported underlying condition, n(%)a | — | 22 (12) | 4/199 (2) |
| Serogroup, n (%) | |||
| C | 156 (49) | 88 (49) | — |
| Y | 139 (43) | 80 (44) | — |
| W | 25 (8) | 13 (7) | — |
| Outcome, n (%) | |||
| Survived | 270 (85) | 156 (87) | — |
| Died | 46 (15) | 23 (13) | — |
| Year, n (%) | |||
| 2006 | 41 (13) | 22 (12) | 25 (13) |
| 2007 | 39 (12) | 24 (13) | 33 (17) |
| 2008 | 25 (8) | 11 (6) | 14 (7) |
| 2009 | 48 (15) | 27 (15) | 34 (17) |
| 2010 | 60 (19) | 41 (23) | 51 (26) |
| 2011 | 45 (14) | 24 (13) | 15 (8) |
| 2012 | 36 (11) | 21 (12) | 20 (10) |
| 2013 | 22 (7) | 11 (6) | 7 (4) |
—, not applicable.
Underlying conditions for controls included cancer (n = 1), diabetes (n = 1), and other immunodeficiency disorder, not specified (n = 2). Underlying conditions for cases included cancer (n = 2), complement deficiency (n = 5), diabetes (n = 3), kidney disease (n = 2), asplenia (n = 1), and other immunodeficiency disorder, not specified (n = 9).
Vaccination status was verified by a provider or the immunization registry for 87% of enrolled case patients and controls; 36 (20%) cases and 87 (44%) controls were vaccinated with a single dose of MenACWY-D (Fig 1). Of the 36 case patients vaccinated with MenACWY-D, 13 were serogroup C, 22 were serogroup Y, and 1 was serogroup W. Among the cases who were unvaccinated, 75 were serogroup C, 58 were serogroup Y, and 12 were serogroup W. Case patients (n = 36) were vaccinated a median of 34 months before disease onset (range, 3 to 77 months). Controls (n = 87) were vaccinated a median of 32 months before disease onset of the matched case (range, 1 to 93 months).
FIGURE 1.
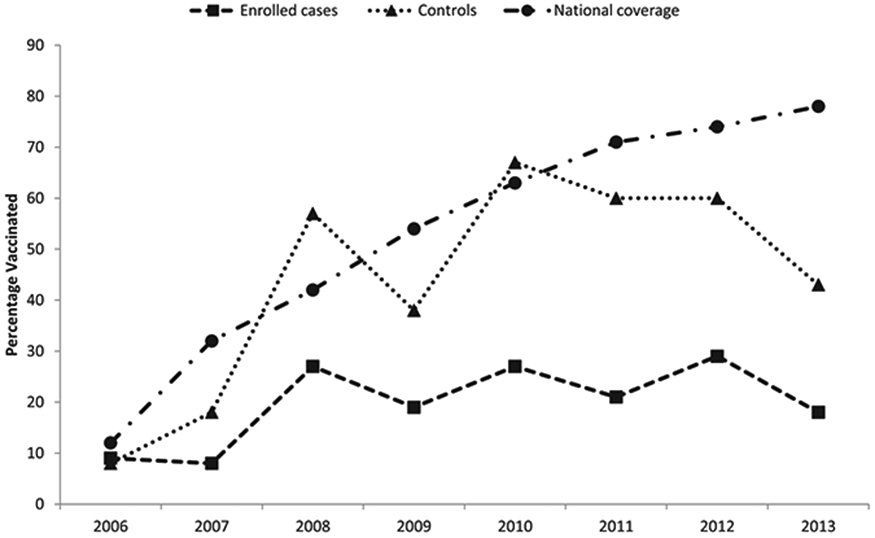
Percent of enrolled cases and controls vaccinated, and vaccination coverage among US teenagers aged 13 to 17 years11, ABCs and MeningNet Sites, 2006 to 2013.
The overall VE of a single dose of MenACWY-D against meningococcal disease caused by serogroups C, Y, or W was 69% (95% confidence interval [CI]: 51% to 80%). Among adolescents with no underlying condition, VE was 71% (95% CI: 54% to 82%). Serogroup C VE was 77% (95% CI: 57%–88%) and serogroup Y VE was 51% (95% CI: 1% to 76%; Table 2). A serogroup W VE could not be calculated because of low sample size. VE was 79% (95% CI: 49% to 91%) in the first year after vaccination, 69% (95% CI: 44% to 83%) at 1 to <3 years, and 61% (95% CI: 25% to 79%) 3 to <8 years after vaccination (Table 3). The GEE model produced point estimates that were not substantially different from those obtained from standard conditional logistic regression but with smaller standard errors (Supplemental Table 5).
TABLE 2.
VE Estimates and Serogroup Specific Estimates, Using the GEE and Controlling for Underlying Medical Conditions and Smoking, ABCs and MeningNet Sites, 2006 to 2013
| VE (95% CI) | |
|---|---|
| All Serogroups (C, Y, and W)a | 69% (51% to 80%) |
| Serogroup C | 77% (57% to 88%) |
| Serogroup Y | 51% (1% to 76%) |
Estimate for serogroup W could not be calculated because of low sample size.
TABLE 3.
VE, by Time Interval Since Vaccination, Using the GEE and Controlling for Underlying Medical Conditions and Smoking, ABCs and MeningNet Sites, 2006 to 2013
| Serogroup C Cases | Serogroup Y Cases | VE (95% CI) | |
|---|---|---|---|
| Vaccinated <1 y | 2 | 3 | 79% (49% to 91%) |
| Vaccinated 1 to <3 y | 7 | 8 | 69% (44% to 83%) |
| Vaccinated 3 to <8 y | 4 | 11 | 61% (25% to 79%) |
DISCUSSION
MenACWY-D was effective against meningococcal disease caused by serogroups C and Y early after vaccination but effectiveness declined over time. A single dose of MenACWY-D did not provide sufficient protection against meningococcal disease 3 to 8 years after vaccination. These estimates are consistent with immunogenicity data that revealed decreasing levels of serum bactericidal antibody 3 to 5 years postvaccination.12,13
Among adolescents and young adults, the risk of meningococcal disease is highest from 16 through 23 years of age. Based on the results of this study, a single dose strategy at 11 to 12 years may not prevent disease during the highest risk period starting at age 16 years. During public discussion of preliminary data from this study at the October 2010 ACIP meeting, the policy options of adding a booster dose at age 16 years or moving the single dose of MenACWY vaccine to age 14 to 15 years were considered. Adding a booster dose of MenACWY at 16 years of age was preferred by ACIP to provide more opportunities to increase vaccination coverage and to continue to protect adolescents ages 11 to 13 years.14 In 2015, nine years after introduction, coverage with a single dose of meningococcal conjugate vaccines among 13- to 17-year-olds was 81.3% and only 33.3% of teenagers 17 years of age had received 2 doses of MenACWY.15 However, even with low coverage with the booster dose, only an estimated 30 to 50 cases of serogroup C and Y meningococcal disease occurred among adolescents aged 18 to 24, which may be an effect of a decline in meningococcal disease rates seen in all ages since before and during implementation of the adolescent program.
The waning VE of MenACWY-D demonstrated in this evaluation is different than previous experience with conjugate vaccines such as pneumococcal and Haemophilus influenzae type b (Hib) vaccine, which have demonstrated long-term protection even though circulating antibody declines.16 The reasons for this are unclear, but 1 key difference is that MenACWY-D uses diphtheria toxoid as the protein carrier. Hib vaccines using diphtheria toxoid as the protein carrier were found to be less effective than other Hib conjugate vaccines when compared among infants.17 MenACWY-D VE is also lower than effectiveness of monovalent serogroup C meningococcal conjugate vaccines in adolescents vaccinated in the United Kingdom, where VE was 93% up to 4 years after vaccination.18 The low effectiveness of the serogroup Y component of the vaccine contributed to the overall reduced effectiveness and likely the limited duration of protection of this multivalent vaccine. As serogroup Y caused almost half of the vaccine-preventable disease in adolescents before vaccine implementation, vaccines that provide protection against serogroup C and Y are important in the United States.3
Conducting a case-control evaluation across multiple states, over several years, and in the adolescent age group was challenging. Many adolescents declined to participate, cases and controls were difficult to contact even with use of mobile telephone numbers when available, and frequently the time interval from case onset to enrollment was long. Moreover, meningococcal disease incidence is low, so our overall sample size is small despite the participation of multiple health departments. Although initially the evaluation period was extended to increase power, the long evaluation period allowed for an assessment of duration of protection. Reporting bias may play a role in underestimating the VE if cases were more likely to be enrolled if they were a vaccination failure; however, unenrolled cases did not have their vaccination status verified so assessing this potential bias is difficult. Although case and control enrollment bias may result in underestimating or overestimating point estimates, bias should not have impacted the finding of waning immunity. The CIs overlap between the time periods measured for VE, but the point estimate and upper limit of the CI is lower in persons vaccinated 3 to 8 years before compared with persons vaccinated <1 year before enrollment.
This evaluation demonstrates the critical need to conduct rigorous and systematic postlicensure VE evaluations to inform immunization policymakers. However, it also highlights the limitations and challenges of case-control studies to evaluate VE where disease incidence before vaccination is very low. Two new serogroup B meningococcal vaccines, licensed for use in 2014 and 2015 in the United States by the Food and Drug Administration after an accelerated approval process, target the serogroup that is not prevented by MenACWY vaccines. However, serogroup B incidence has declined over the past decade and is lower in adolescents than serogroups C and Y disease before the MenACWY vaccine recommendations. In February 2015, ACIP recommended serogroup B meningococcal vaccines for persons at increased risk for meningococcal disease, and in June 2015, ACIP recommended that a serogroup B meningococcal vaccine series may be administered to adolescents and young adults aged 16 to 23 years to provide short-term protection against most strains of serogroup B meningococcal disease.19,20 Implementation of serogroup B vaccination is likely to be highly variable given the recommendation allows for individual clinical decision, the target age group is late adolescence, and the vaccines are multidose series. Therefore, monitoring vaccine impact and effectiveness of these vaccines, although important to inform future decisions around serogroup B vaccine use, will be especially challenging.
CONCLUSIONS
We found that MenACWY-D was effective but that protection waned rapidly over time. These results cannot be extrapolated to other quadrivalent meningococcal conjugate vaccines licensed in the United States and other countries. Although MenACWY-D was originally licensed as a single dose among 2- through 55-year-olds, a booster dose was added to the indication in August 2014, on the basis of a phase 4 safety and immunogenicity evaluation, which revealed a stronger immunogenicity response after the booster dose. A second dose should provide longer duration of protection in individuals compared with a single dose; providers should ensure their adolescent patients are vaccinated with 1 of the MenACWY vaccines after their 16th birthday to optimize protection as they enter the age of highest risk. However, given the current low disease burden among adolescents despite low coverage with the booster dose, the additional impact gained from the booster dose in terms of cases prevented is likely to be limited.
Supplementary Material
WHAT’S KNOWN ON THIS SUBJECT:
Because meningococcal disease incidence is low, prelicensure randomized controlled trials of meningococcal (groups A, C, W, and Y) polysaccharide conjugate vaccines used evidence of serologic protection rather than clinical end points. Early estimates of meningococcal (groups A, C, W, and Y) polysaccharide diphtheria toxoid conjugate vaccine (MenACWY-D) effectiveness suggested immunity may wane several years after a single dose.
WHAT THIS STUDY ADDS:
This case-control vaccine effectiveness study of a meningococcal conjugate vaccine product (MenACWY-D) was conducted over several years and demonstrates serogroup-specific effectiveness and duration of protection. Preliminary data from this study informed the policy decision to add a booster dose at age 16 years.
ACKNOWLEDGMENTS
The Active Bacterial Core Surveillance Team includes: Mirasol Apostol, Pam Daily Kirley, Nima Harandi, Maria Rosales, Emilia Basilio, and Joelle Nadle (California Emerging Infections Program); Ken Gershman, Lisa Miller, Deborah Aragon, and Denise-Woods Stout (Colorado Emerging Infections Program); Matt Cartter (Connecticut Emerging Infections Program); Monica Farley and Melissa Tobin-D’Angelo (Georgia Emerging Infections Program); Mary Messenger, Angela Badcon, Amanda Palmer, Laurie Sanza, Alicia Schmidt, and Rosemary Hollick (Maryland Emerging Infections Program); Jean Rainbow, Catherine Lexau, Richard Danila, Craig Morin, Lori Triden, Brenda Jewell, and Billie Junie (Minnesota Emerging Infections Program); Megin Nichols (New Mexico Emerging Infections Program); Nancy Bennett (New York Emerging Infections Program); Ann Thomas, Mark Schmidt, Jamie Thompson, and Tasha Poissant (Oregon Emerging Infections Program); Brenda Barnes and Katie Dyer (Tennessee Emerging Infections Program).
The MeningNet Partners include: Sherri Davidson and Ana Oliveira (Alabama Department of Public Health); Clarisse A. Tsang, Susan Goodykoontz, Linda Getsinger, Karman Tam, Shoana M. Anderson, Stephanie Kreis, and Daniel Williamson (Arizona Department of Health Services); Rosie Glenn-Finer, John Semerdjian, Lee St Pierre, Kathleen Winter, Kathleen Harriman, Jessica Atwell, and Margot Graves (California Department of Public Health); Kristin Short and Nathan Wang (Houston Health Department); Kate Goodin, Heather Parth, and Avalon Adams-Thames (Florida Department of Health); Dana Greenwood and Christine Feaster (Indiana State Department of Health); Ann Garvey and Diana L. Von Stein (Iowa Department of Public Health); Ann Farmer, Megan Kelly, and Heidi Dragoo (Maine Department of Health and Human Services); Will Lapsley and Melissa Cumming (Massachusetts Department of Public Health); Cindy Allard and Mary Jane Coleman (Mississippi Department of Health); Jody Schweitzer and Jane Manning (New Hampshire Department of Health and Human Services); Mike Antwi, Paula E. Del Rosso, Marie Dorsinville, Perminder Khosa, Linda Steiner-Sichel, and Don Weiss (New York City Department of Health and Mental Hygiene); Zack Moore (North Carolina Department of Health and Human Services); Perianne Lurie (Pennsylvania Department of Health); Jennifer Gutowski, Ami Patel, Jessica Savage, and Crystal Witherspoon (Philadelphia Department of Public Health); Dana Giurgiutiu, Gerhild Ulman, and Shirley Jankelovich (South Carolina Department of Health and Environmental Control); Brenda Rue (Tennessee Department of Health); Tamara Baldwin, Neil Pascoe, and Barbara Scaife (Texas Department of State Health Services); Azadeh Tasslimi and Chas DeBolt (Washington State Department of Health); Stephanie McLemore (West Virginia Department of Health and Human Resources); Anna Kocharian and Susann Ahrabi-Fard (Wisconsin Department of Health Services).
The authors also thank Carolyn Wright, Londell McGlone, Emily Weston, Tami Skoff, Martha Iwamoto, Kim Cushing, Chris Van Beneden, Karrie-Ann Toews, Shani Doss, Amy Blain, Gayle Langley, Thomas Clark, and Stacey Martin (Centers for Disease Control and Prevention) for their support for this evaluation.
FUNDING:
This study was supported by funding from the Centers for Disease Control and Prevention through the Emerging Infections Program and the Epidemiology and Laboratory Capacity Cooperative Agreements.
ABBREVIATIONS
- ABCs
Active Bacterial Core surveillance
- ACIP
Advisory Committee on Immunization Practices
- CDC
Centers for Disease Control and Prevention
- CI
confidence interval
- GEE
generalized estimating equation
- Hib
Haemophilus influenzae type b
- MenACWY
meningococcal (groups A, C, W, and Y) polysaccharide conjugate vaccine
- MenACWY-CRM
meningococcal (groups A, C, W, and Y) oligosaccharide diphtheria CRM197 conjugate vaccine
- MenACWY-D
meningococcal (groups A, C, W, and Y) polysaccharide diphtheria toxoid conjugate vaccine
- PCR
polymerase chain reaction
- VE
vaccine effectiveness
Footnotes
POTENTIAL CONFLICT OF INTEREST: Dr Schaffner is a member of Data Safety Monitoring Boards for Merck and Pfizer and a consultant for Dynavax, Novavax, Genentech and Sanofi Pasteur; the other authors have indicated they have no potential conflicts of interest to disclose.
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
Reprints Information about ordering reprints can be found online: http://www.aappublications.org/site/misc/reprints.xhtml
REFERENCES
- 1.Cohn AC, MacNeil JR, Clark TA, et al. ; Centers for Disease Control and Prevention (CDC). Prevention and control of meningococcal disease: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2013;62(RR-2):1–28 [PubMed] [Google Scholar]
- 2.Adams DA, Jajosky RA, Ajani U, et al. ; Centers for Disease Control and Prevention (CDC). Summary of notifiable diseases--United States, 2012. MMWR Morb Mortal Wkly Rep. 2014;61(53):1–121 [PubMed] [Google Scholar]
- 3.Cohn AC, MacNeil JR, Harrison LH, et al. Changes in Neisseria meningitidis disease epidemiology in the United States, 1998-2007: implications for prevention of meningococcal disease. Clin Infect Dis. 2010;50(2):184–191 [DOI] [PubMed] [Google Scholar]
- 4.Caugant DA, Høiby EA, Magnus P, et al. Asymptomatic carriage of Neisseria meningitidis in a randomly sampled population. J Clin Microbiol. 1994;32(2):323–330 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Christensen H, May M, Bowen L, Hickman M, Trotter CL. Meningococcal carriage by age: a systematic review and meta-analysis. Lancet Infect Dis. 2010;10(12):853–861 [DOI] [PubMed] [Google Scholar]
- 6.Harrison LH, Shutt KA, Arnold KE, et al. Meningococcal carriage among Georgia and Maryland high school students. J Infect Dis. 2015;211(11):1761–1768 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.MacNeil JR, Cohn AC, Zell ER, et al. Early estimate of the effectiveness of quadrivalent meningococcal conjugate vaccine. Pediatr Infect Dis J. 2011; 30(6):451–455 [DOI] [PubMed] [Google Scholar]
- 8.Schuchat A, Hilger T, Zell E, et al. ; Active Bacterial Core Surveillance Team of the Emerging Infections Program Network. Active bacterial core surveillance of the emerging infections program network. Emerg Infect Dis. 2001;7(1):92–99 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mothershed EA, Sacchi CT, Whitney AM, et al. Use of real-time PCR to resolve slide agglutination discrepancies in serogroup identification of Neisseria meningitidis. J Clin Microbiol. 2004;42(1):320–328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lin IF, Lai MY, Chuang PH. Analysis of matched case-control data with incomplete strata: applying longitudinal approaches. Epidemiology. 2007;18(4):446–452 [DOI] [PubMed] [Google Scholar]
- 11.Elam-Evans LD, Yankey D, Jeyarajah J, et al. National, regional, state, and selected local area vaccination coverage among adolescents aged 13-17 years–United States, 2013. MMWR Morb Mortal Wkly Rep. 2014;63(29):625–633 [PMC free article] [PubMed] [Google Scholar]
- 12.Gill C, Reisinger K, Block S, Izu A, Odrljin T, Dull PM. Antibody persistence and booster response of a quadrivalent meningococcal conjugate vaccine in adolescents. J Pediatr. 2014;164(6):1409–1415 [DOI] [PubMed] [Google Scholar]
- 13.Gill CJ, Baxter R, Anemona A, Ciavarro G, Dull P. Persistence of immune responses after a single dose of Novartis meningococcal serogroup A, C, W-135 and Y CRM-197 conjugate vaccine (Menveo®) or Menactra® among healthy adolescents. Hum Vaccin. 2010;6(11):881–887 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Centers for Disease Control and Prevention (CDC). Licensure of a meningococcal conjugate vaccine for children aged 2 through 10 years and updated booster dose guidance for adolescents and other persons at increased risk for meningococcal disease--Advisory Committee on Immunization Practices (ACIP), 2011. MMWR Morb Mortal Wkly Rep. 2011;60(30):1018–1019 [PubMed] [Google Scholar]
- 15.Reagan-Steiner S, Yankey D, Jeyarajah J, et al. National, Regional, State, and Selected Local Area Vaccination Coverage Among Adolescents Aged 13-17 Years - United States, 2015. MMWR Morb Mortal Wkly Rep. 2016;65(33):850–858 [DOI] [PubMed] [Google Scholar]
- 16.Pollard AJ, Perrett KP, Beverley PC. Maintaining protection against invasive bacteria with protein-polysaccharide conjugate vaccines. Nat Rev Immunol. 2009;9(3):213–220 [DOI] [PubMed] [Google Scholar]
- 17.Decker MD, Edwards KM, Bradley R, Palmer P. Comparative trial in infants of four conjugate Haemophilus influenzae type b vaccines. J Pediatr. 1992;120(2 pt 1):184–189 [DOI] [PubMed] [Google Scholar]
- 18.Trotter CL, Andrews NJ, Kaczmarski EB, Miller E, Ramsay ME. Effectiveness of meningococcal serogroup C conjugate vaccine 4 years after introduction. Lancet. 2004;364(9431):365–367 [DOI] [PubMed] [Google Scholar]
- 19.Folaranmi T, Rubin L, Martin SW, Patel M, MacNeil JR; Centers for Disease Control (CDC). Use of Serogroup B Meningococcal Vaccines in Persons Aged ≥10 Years at Increased Risk for Serogroup B Meningococcal Disease: Recommendations of the Advisory Committee on Immunization Practices, 2015. MMWR Morb Mortal Wkly Rep. 2015;64(22):608–612 [PMC free article] [PubMed] [Google Scholar]
- 20.MacNeil JR, Rubin L, Folaranmi T, Ortega-Sanchez IR, Patel M, Martin SW. Use of Serogroup B Meningococcal Vaccines in Adolescents and Young Adults: Recommendations of the Advisory Committee on Immunization Practices, 2015. MMWR Morb Mortal Wkly Rep. 2015;64(41):1171–1176 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.