
Fig. 4.
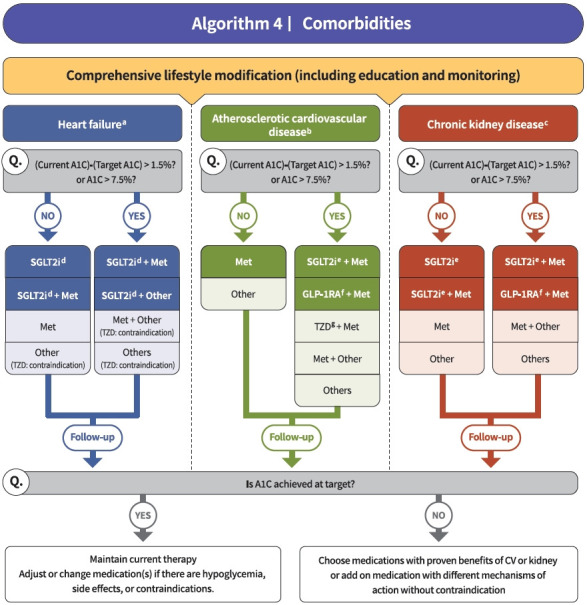
Treatment algorithm 4 (comorbidities) for patients with type 2 diabetes mellitus who have heart failure (HF), established atherosclerotic cardiovascular disease (eASCVD), or chronic kidney disease (CKD). If patients have underlying above comorbidities, glucose-lowering agents, including sodium-glucose cotransporter 2 (SGLT2) inhibitor or glucagon-like peptide-1 receptor agonist (GLP1-RA), are the preferred choice. For patients with HF, glucose-lowering agents, including SGLT2 inhibitors with proven cardiovascular (CV) benefits, should be prioritized. Regimens that include SGLT2 inhibitors or GLP-1RAs with proven CV benefits should be prioritized for combination therapy in patients with eASCVD. For patients with albuminuria or reduced estimated glomerular filtration rate (eGFR), glucose-lowering agents, including SGLT2 inhibitors with proven renal and CV benefits, should be prioritized. A1C, glycosylated hemoglobin; Met, metformin; TZD, thiazolidinedione. aParticularly HF with reduced ejection fraction (HFrEF, clinical diagnosis of HF and left ventricular ejection fraction ≤40%), bHistory of acute coronary syndrome or myocardial infarction, stable or unstable angina, coronary heart disease with or without revascularization, other arterial revascularization, stroke, or peripheral artery disease assumed to be atherosclerotic in origin, ceGFR <60 mL/min/1.73 m2 or urine albumin creatinine ratio ≥30 mg/g, dDapagliflozin, empagliflozin, ertugliflozin, eDapagliflozin, empagliflozin, fDulaglutide, liraglutide, semaglutide, gPioglitazone.