
Figure 1.
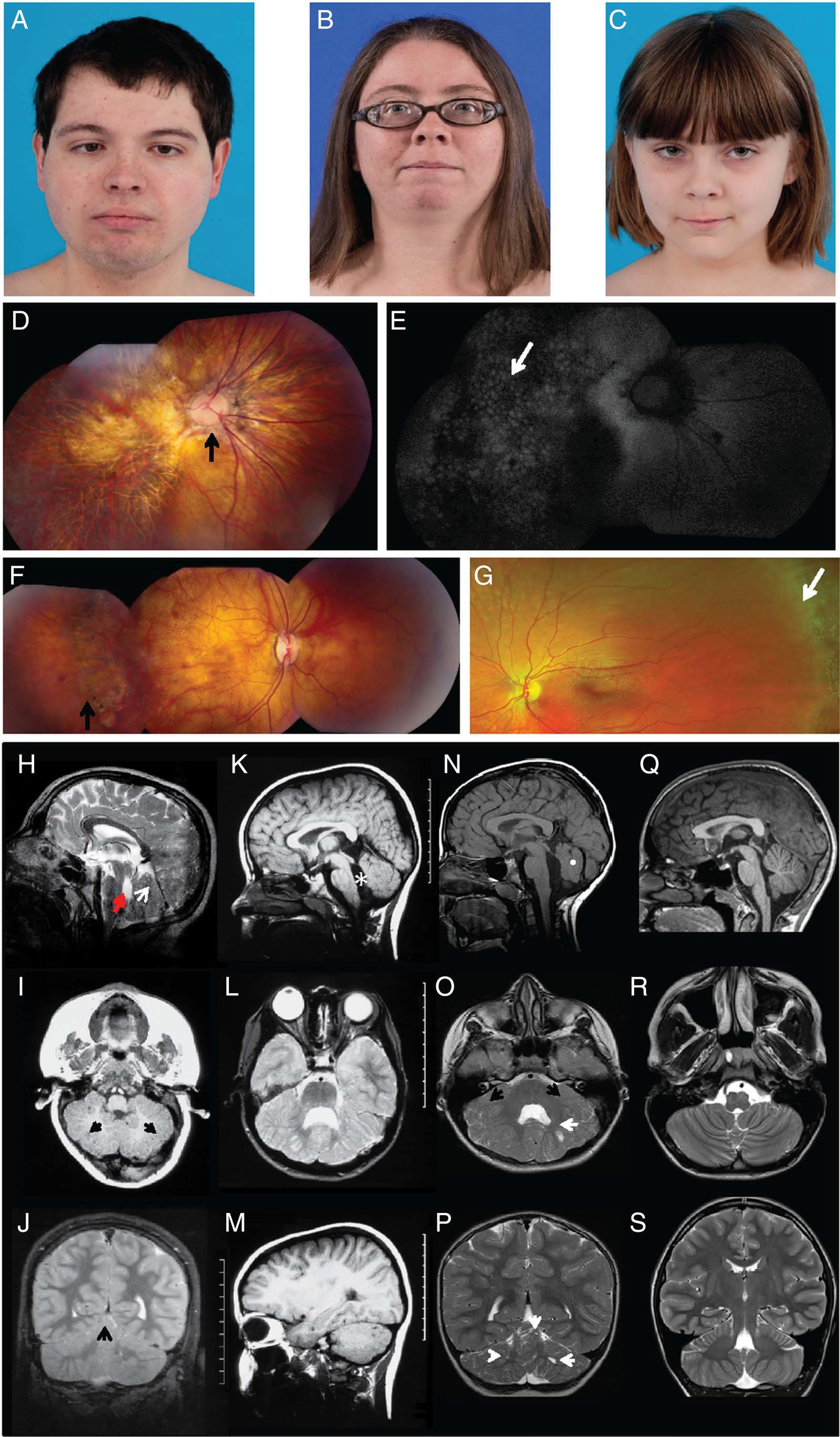
Clinical and neuroimaging features of patients with LAMA1 mutations. (A) Clinical features of patients showing distinct ophthalmologic characteristics. Patients 1 (A), 2 (B) and 3 (C) had unremarkable facial features. Note residual strabismus of patient 1 after corrective surgery. (D) Composite colour fundus photography of patient 1’s right eye demonstrating a dysplastic optic nerve with nasalised retinal vasculature (arrow) and diffuse chorioretinal atrophy involving the macula and midperiphery. (E) Composite fundus autofluorescence of the same eye, showing a ‘cobblestone’ pattern (arrow) indicating chorioretinal atrophy. (F) Composite colour fundus photograph of patient 2, the older sister of patient 1, showing moderate chorioretinal atrophy (arrow). (G) Colour fundus photo of patient 3 showing normal-appearing posterior pole and peripheral lattice degeneration (arrow), despite only mild myopia. (H–S) Brain MRI demonstrates cerebellar dysplasia associated with cysts. Brain MRI findings of patient 1 (H–J), patient 2 (K–M), patient 3 (N–P) and a healthy control (Q–S) are shown. (H) Patient 1 at 7 months of age has multiple cortical/subcortical cysts in the cerebellar vermis (arrow), dysplastic cerebellar vermis and enlarged fourth ventricle (arrowhead) with an abnormal rectangle-like shape (midsagittal-T1). The midbrain is mildly elongated, and the pons is mildly reduced in size. (I) Subcortical cysts (arrows) and dysplasia are also seen in the cerebellar hemispheres (axial-T1). (J) At 10 years 7 months, dysplasia in cerebellar vermis and hemispheres with multiple cortical and subcortical cysts (arrow) remain visible. (K) Patient 2 has hypoplasia and dysplasia of the cerebellar vermis with cortical and subcortical cysts, enlarged fourth ventricle (asterisk), elongated midbrain and pons appearing small (midsagittal-T1). (L) Cerebellar hemispheres are dysplastic and with multiple cortical and subcortical cysts in patient 2 (axial-T2). (M) Cortical and subcortical cysts within the left cerebellar hemisphere of patient 2 (parasagittal-T1) are shown. Images (K–M) were taken at age 6 years and 10 months. (N) Patient 3 has a normal sized but severely dysplastic vermis (white dot) with lack of separation of the vermian lobules (midsagittal-T1). Axial (O) and coronal (P) T2-weighted images of patient 3 show a markedly dysplastic appearance of the cerebellar hemispheres and the vermis with a diffusely abnormal configuration of the cerebellar folia and sulci (black arrows). Multiple small cysts are noted in the cerebellar hemispheres bilaterally (white arrows). Images (N–P) were taken at 4 years 3 months. (Q) A healthy 12-year-old control with normal anatomy of the posterior fossa structures (midsagittal-T1) and a normal triangle-shaped fourth ventricle is shown. Normal morphology of the cerebellum with an ‘onion-like’ foliation/fissuration pattern and white matter arborisation in the cerebellar hemispheres seen in axial (R) and coronal (S) T2 weighted images.