
Figure 2.
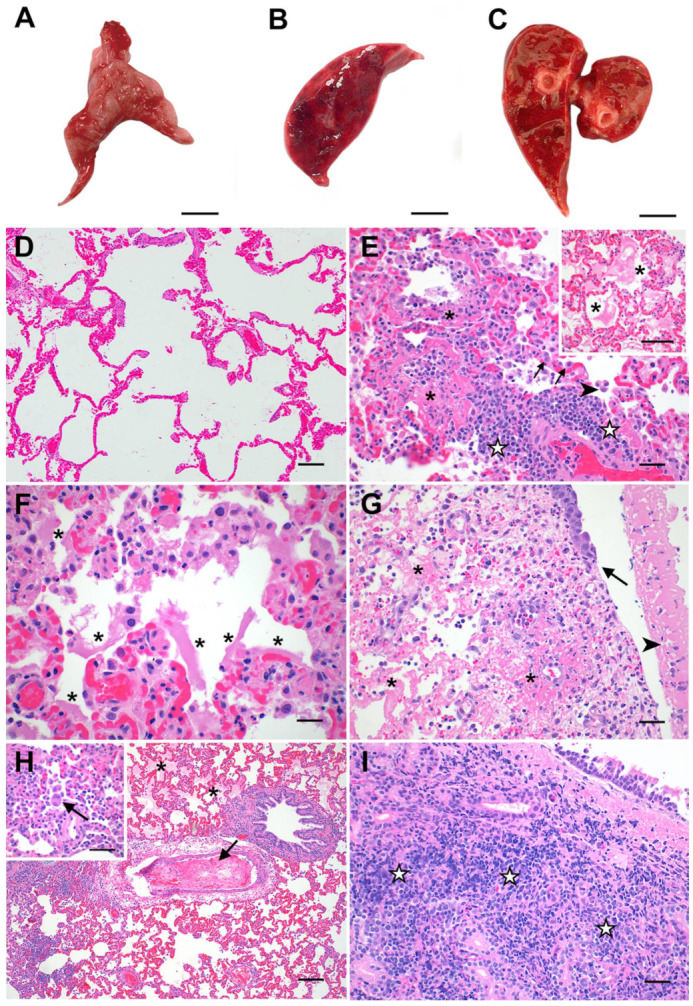
Pathologic features of acute SARS-CoV-2 infection in cats are analogous to the exudative phase of COVID-19. Compared to lungs from healthy sham-inoculated cats (A), the lungs of SARS-CoV-2-infected cats were diffusely consolidated, dark red, and edematous at both 4 dpi (B) and 8 dpi (C). The lungs of healthy, uninfected cats (D) were histologically normal, with open alveoli and minimal atelectasis. At 4 dpi, the lungs of SARS-CoV-2-infected cats (E) exhibited discrete foci of alveolar inflammation and necrosis with fibrin deposition (✱), increased alveolar macrophages (arrowhead), perivascular lymphocytes (☆), and type II pneumocyte hyperplasia (arrows). The alveoli in these cats’ lungs were frequently filled with large amounts of edema and fibrin strands ((E) inset), and there were multifocal areas of hyaline membrane formation (F) (✱). The distal trachea of one SARS-CoV-2-infected cat (G) was multifocally ulcerated at 4 dpi (arrow) with diphtheritic membrane formation (arrowhead) and multifocal areas of submucosal necrosis and fibrinoid vasculitis (✱). At 8 dpi (H), fibrinoid vasculitis, vascular thrombosis (arrow), and occasional syncytial cells (H inset) were observed in addition to the histopathologic changes described above. Tracheal lesions observed at 8 dpi (I) were characterized by varying degrees of lymphoplasmacytic, histiocytic, and neutrophilic inflammation, with multifocal areas of submucosal necrosis. Magnification: (A–C) scale bar = 1 cm; (D,H) 10×, scale bar = 100 µm; (E) 20×, scale bar = 50 µm; ((E) inset, (G), (H) inset, (I)) 40×, scale bar = 25 µm; (F) 60×, scale bar = 17 µm.