
Fig. 3.
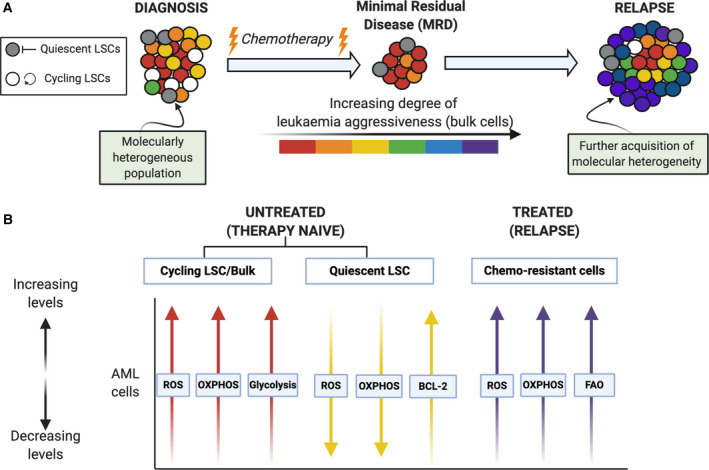
Schematic representation of cellular and metabolic changes in adult AML following chemotherapy. (A) At diagnosis, AML comprises a molecularly heterogeneous population of cycling and quiescent LSCs and bulk AML blast cells. Treatment with conventional chemotherapy often results in complete remission; however, there many remain small numbers of leukaemic cells that are chemoresistant giving rise to what is termed ‘minimal residual disease’ (MRD). The MRD chemotherapy‐resistant LSC population possess the ability to re‐initiate leukaemia and potentiate disease aggressiveness through further acquisition of molecular heterogeneity. (B) The associated metabolic programmes of LSCs and bulk cells are dynamic and vary based upon therapy status. Initially, both therapy‐naïve quiescent and cycling LSCs are highly sensitive to chemotherapy: Therapy‐naïve quiescent LSCs have low ROS levels and OXPHOS dependent on high BCL‐2 levels when compared to cycling LSCs and bulk AML cells, of which also depend on aerobic glycolysis. Cells which remain postchemotherapy, therapy‐resistant, have notably higher ROS levels, high OXPHOS and FAO when compared to therapy‐naïve AML cells.