
FIGURE 1.
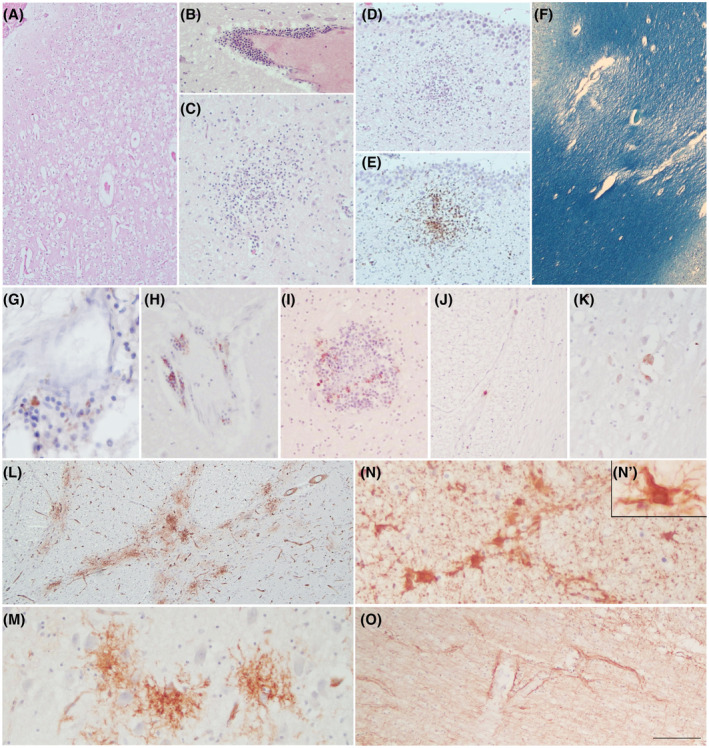
COVID‐19 neuropathology. H&E reveals diffuse cortical oedema (A), inflammatory perivascular infiltrates (B), and micro nodules in the basal ganglia (C) and subependymal zone (D), which are also identified with CD68 marker (E). LFB shows myelin loss in the subcortical WM due to SVD (F). Rare foci of perivascular T‐lymphocytes (G) and B‐lymphocytes (H) are identified using anti‐CD3 and anti‐CD20 antibodies, respectively. B‐lymphocytes are also observed within some inflammatory nodules (I). Rare SARS‐Cov‐2 positive cells are detected only in the lower brainstem of the one case (Cov3) (J, K).CD34 staining displays foci of abnormal tuft‐like capillary features, particularly frequent in the pons (L, M). GFAP reveals mild to moderate gliosis with frequent reactive astrocytes (N, N’). GFAP enhancement in astrocytic end feet around blood vessels is a peculiar picture (O). Scale bars: 512 μm (F); 288 μm (A, L); 180 μm (D, E); 106 μm (B, J, O); 76 μm (C, I); 47 μm (H, K, M, N); 31 μm (G); 17 μm (N’)