
Figure 2.
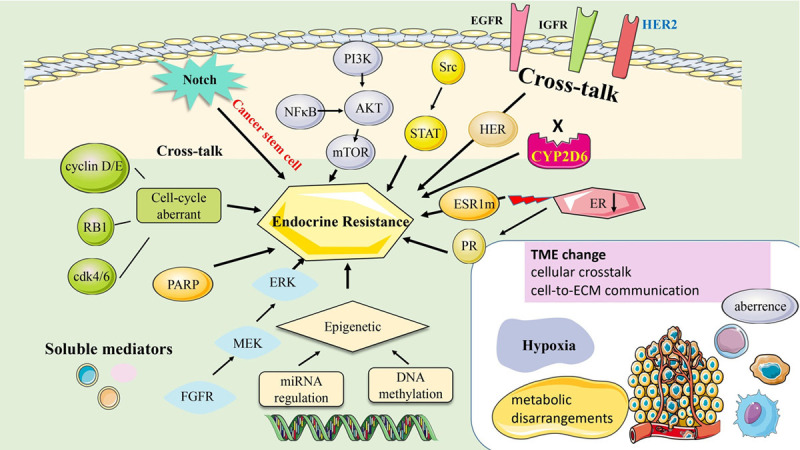
The mechanism of endocrine resistance in Hormone-positive breast cancer. A. ER down regulation (such as CYP2D6 variants; lack of ERα expression). B. The profiles of DNA methylation or miRNA regulation with differential adaptation of breast cancer cells to the hormone therapy, and hence could be cause of hormone resistance. C. Tumors harboring mutations of ESR1. D. Cross-talk between ER and other signaling networks, such as HER2/IFGR/EGFR/MAPK/mTOR). Acquired resistance to endocrine therapy involves alterations in translation signals through increasing the expression and activity of tyrosine kinase receptor family proteins (HER2, EGFR, and IGFR). These events result in aberrant activation of cAMP/PKA, MAPK/ERK, and PI3K/AKT signaling pathways. E. Aberrance of cell cycle regulators (c-myc; cyclin D1/E; CDK4/6). F. Resistance from Cancer stem cell: breast cancer stem cells to generate resistant BCs containing part of BCSCs; the other is via the dedifferentiation of BCs will gnerate tumors resistant to endocrine therapy and leading to the acquisition of BCSCs. G. Resistance from tumor microenvironment (cellular crosstalk and cell-to-ECM communication, inducing the release of soluble factors in charge of immune evasion and ECM remodeling, which further promote therapy resistance. Abbreviations: ER, Estrogen receptor; ECM, Extracellular Matrix; ESR1, Estrogen Receptor 1; EGFR, epidermal growth factor receptor; FGF2, fibroblast growth factor 2; FGFR, fibroblast growth factor receptor; GFR, growth factor receptor; HER2, human epidermal growth factor receptor 2; IGF, insulin-like growth factor; IGFR, insulin-like growth factor 1 receptor; MAPK, mitogen-activated protein kinase; mTOR, mammalian target of rapamycin; PI3K, phosphatidylinositol 3 kinase; PR, Progesterone receptor; TME, tumor microenvironment.