
Figure 4. Images of Abnormalities in 4 Cases With Presentations Suggestive of Neuroinflammatory Disease at or Near the Time of Brain Biopsy.
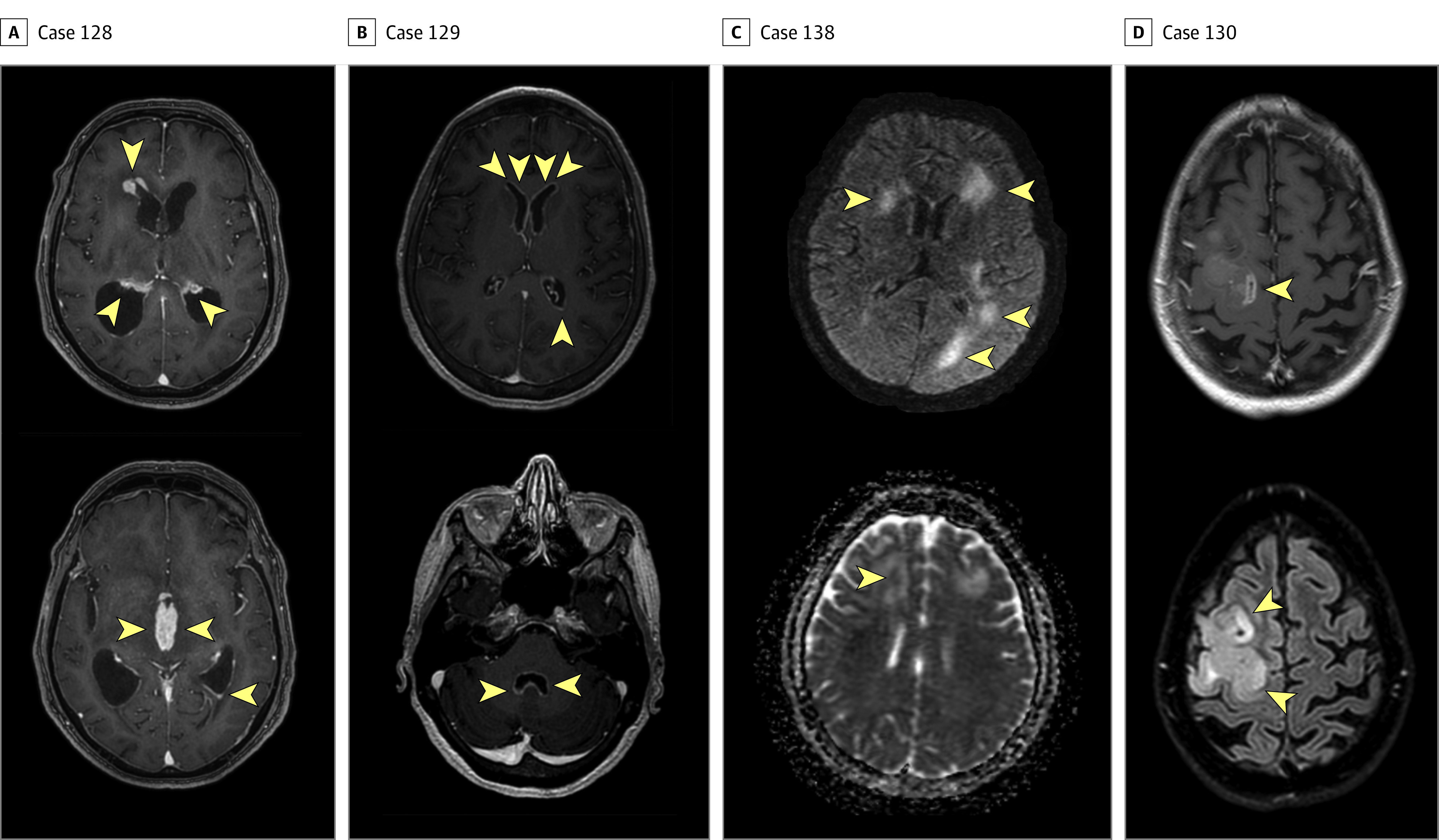
A, In case 128, postcontrast T1-weighted images demonstrate thick areas of enhancement along nearly all ependymal surfaces, including the lateral ventricles (top image), third ventricle (bottom image), and fourth ventricle, resulting in acute hydrocephalus. The imaging appearance was believed to be consistent with disseminated tuberculosis and less likely to be lymphoma because of limited restricted diffusion. The final diagnosis was primary central nervous system (CNS) lymphoma. B, In case 129, postcontrast T1-weighted images demonstrate extensive, thin ependymal enhancement along the lateral ventricles (top image) and fourth ventricle (bottom image), with minimal adjacent signal abnormality in the parenchyma. The imaging appearance was believed to be most consistent with infectious ventriculitis and less likely to be carcinomatosis. The final diagnosis was melanoma. C, In case 138, motion-degraded T2-weighted fluid attenuated inversion recovery (T2/FLAIR; top image) image and apparent diffusion coefficient (bottom image) demonstrate asymmetric white matter signal abnormality with variable foci of mildly restricted diffusion. In this immunocompromised patient, images were believed to be potentially consistent with progressive multifocal leukoencephalopathy. The final diagnosis was intravascular lymphoma. D, In case 130, postcontrast T1-weighted (top image) and T2/FLAIR (bottom image) sequences demonstrate expansile signal abnormality with areas of heterogeneous enhancement. Glioblastoma was diagnosed using brain biopsy. Arrowheads indicate areas of abnormalities.