
Fig. 2. Cases of autopsy-confirmed Parkinson’s disease (PD) and progressive supranuclear palsy (PSP).
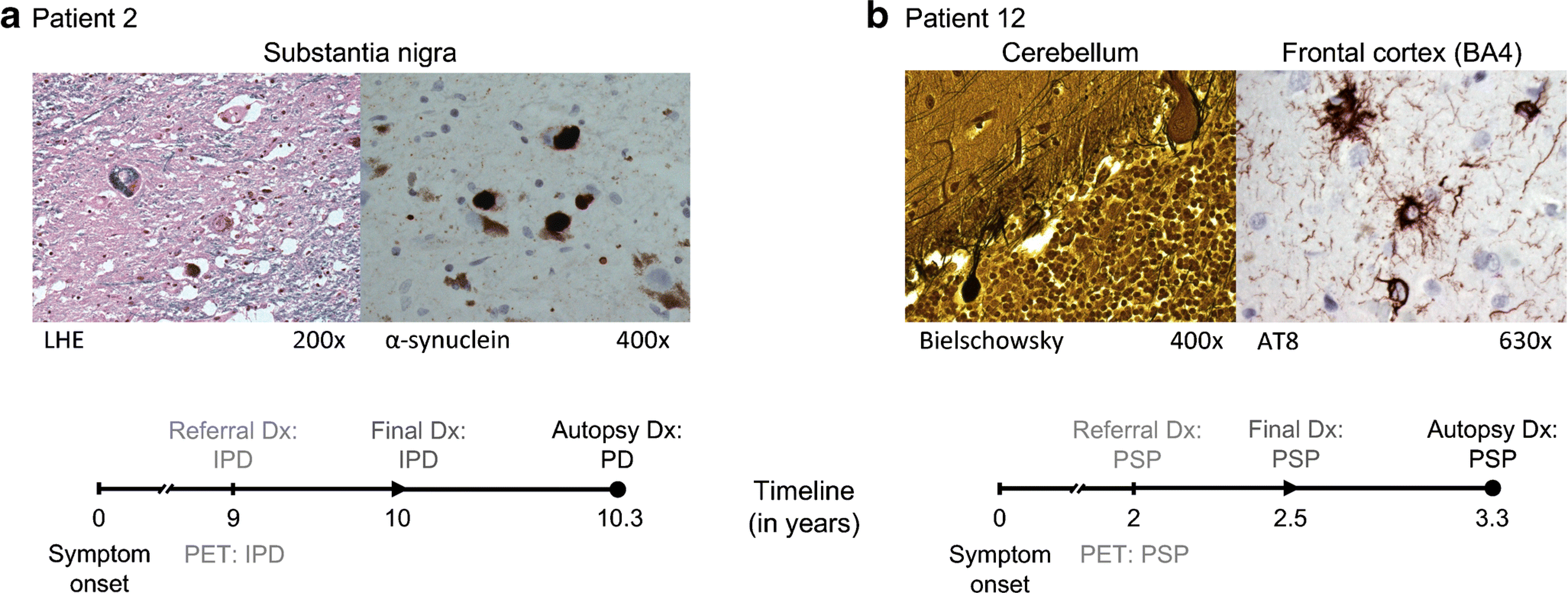
(a) Patient 2 (57-year old male) had an uncertain clinical diagnosis of idiopathic Parkinson’s disease (IPD) at the time of PET referral, roughly 9 years after symptom onset. The automated imaging algorithm classified the patient as IPD (99% likelihood). One year after imaging, a final clinical diagnosis of IPD was reached, which was confirmed on autopsy 4 months later. The neuropathological examination demonstrated Lewy body-containing neurons and severe neuronal loss in the pars compacta of the substantia nigra (LHE, 200×; left). Lewy body-containing neurons were labeled with α-synuclein (400×; right). [LHE=Luxol fast blue hematoxylin and eosin]. (b) At the time of PET referral, Patient 12 (69 years old, male, symptom duration 2 years) had an uncertain clinical diagnosis with PSP as the leading possibility. The automated imaging algorithm classified the patient as PSP (83.3% likelihood). Six months after imaging, a final clinical diagnosis of PSP was made, which was confirmed on autopsy 10 months later. The histopathological examination showed neuronal loss in the globus pallidus, substantia nigra, red nucleus, subthalamic nucleus, pons, medulla oblongata, and cerebellum. The cerebellar cortex displayed loss of Purkinje cells and presence of torpedoes (Bielschowsky, 400×; left). AT8-labeled cells including tufted astrocytes and glial cytoplasmatic inclusions were found in the paracentral cortex (630×; right), superior parietal lobe, and prefrontal cortex.