

Abstract
Objective:
The Illness Identity model posits that self-stigma reduces hope and self-esteem among persons with severe mental illnesses, impacting a range of outcomes. The “insight paradox” anticipates that the negative effects of self-stigma are amplified by insight. This study tested these predictions using both cluster and path analyses.
Method:
117 participants meeting criteria for schizophrenia-spectrum disorders completed measures of self-stigma, self-esteem, hopelessness, insight, social functioning, coping, and symptoms.
Results:
Cluster analysis supported the insight paradox; persons with low self-stigma/high insight had fewer psychiatric symptoms and better interpersonal functioning than persons with high self-stigma/low insight. Path analysis did not support the insight paradox, but indicated that self-stigma and insight impact different outcomes.
Discussion:
Findings suggest that support for the predictions of the Illness Identity model and insight paradox are supported may depend on analytic method.
Conclusions:
Finding suggest that the benefits of self-stigma reduction may be constrained by insight.
Keywords: Illness Identity, Insight Paradox, Self-Stigma, Recovery, Schizophrenia
Research has consistently documented that many diagnosed with psychiatric disorders experience self-stigma, defined as occurring when people diagnosed with mental illness believe that negative stereotypes directed at their group are true of them (e.g., I am incompetent, dangerous, etc., because I have a mental illness) (Corrigan & Watson, 2002). In a review of 80 articles with over 25,000 participants, Dubreucq, Plasse and Franck (2021) found that 35% of persons diagnosed with schizophrenia-spectrum disorders and 31% of persons diagnosed with mental illness overall demonstrated elevated self-stigma.
The facilitation of recovery has become an organizing principle for the mental health field in the past 25 years. Although researchers, clinicians and advocates disagree about whether “outcome” or “process” components of recovery are most important, a consensus is emerging that recovery is a multidimensional construct with both subjective (e.g., self-esteem, hopefulness, meaning in life) and objective (e.g., symptom experience, interpersonal relationships and work) components (Leamy et al., 2011). As self-stigma has been the subject of increasing study, its broad relationships with multiple outcomes related to both the subjective and objective dimensions of recovery have been revealed (Livingston & Boyd, 2010). In their initial discussion of the impact of self-stigma on people diagnosed with severe mental illness, Corrigan and Watson (2002) predicted that elevated self-stigma would be associated with diminished self-esteem and self-efficacy. An attempt to further articulate how self-stigma can come to deeply disrupt a person’s life is the “Illness Identity” model (Yanos, Roe, & Lyaker, 2010). This model posits that self-stigma can degrade a person’s identity, reduce hope and self-esteem, and lead one to believe that there is no possibility for recovery. These negative appraisals are hypothesized to be amplified by the “insight paradox” (Lysaker, Roe & Yanos, 2007), which predicts that an individual’s hope and self-esteem are more negatively impacted when one both identifies as having a mental illness (that is, demonstrates “insight” as typically conceived) and also strongly associates it with negative stereotypes (characteristic of self-stigma). Hopelessness and low self-esteem can also then increase risk for suicide and decrease social interaction. This, in turn, leaves individuals more isolated, coping more passively with symptoms and stressors, limiting engagement in support services. As individuals use more avoidant coping strategies, they are less likely to even try to obtain work, which can further decrease social interactions. Finally, avoidant coping is hypothesized to decrease service engagement and vocational functioning while increasing social isolation, which may all increase symptom severity. Note that the “social-cognitive model” for the effects of self-stigma, proposed by Muňoz and colleagues (Muňoz et al., 2011), made similar predictions regarding the effects of self-stigma on a range of outcomes.
To date, findings from a growing body of research have largely supported most of the components of the Illness Identity model in isolation (see Yanos, DeLuca, Roe, & Lysaker, 2020, for a review), although the “insight paradox,” has been inconsistently supported. Specifically, 9 of 14 studies found support for a moderating effect of self-stigma and insight on outcomes relevant to the Illness Identity model (Yanos et al., 2020). Although sample characteristics (diagnosis and geographic location) were not associated with a likelihood of finding support for the insight paradox, it is possible that methodological approaches did, as some studies used cluster analysis to examine moderation effects, while others used some form of product-term moderation analysis. It is plausible that analytic approach used might partly explain discrepancies in findings, as product-term moderation analysis might be less appropriate for detecting non-linear patterns in moderation. For example, this could occur if high levels of self-stigma are associated with diminished interpersonal functioning when insight is both very high and very low, but not when it is moderate. Another distinction between these approaches is that cluster analysis is regarded as a “person-centered” analysis (i.e., one that uses mathematical algorithms to examined how variables combine across individuals) while other commonly used approaches such as path analysis are regarded as “variable-centered” (i.e., ones that examine relationships between variables) (see von Eye & Bogat, 2006, for an overview of these approaches and their differences). Research in other domains has found that discrepant findings can sometimes emerge when the same data is analyzed using both approaches (Bamaca-Colbert & Gayles, 2010).
Another limitation of the existing research noted by Yanos et al.’s (2020) review is that studies have rarely tested multiple components of the Illness Identity model in the same study. There is also an absence of investigations examining how different analytic approaches (e.g., person-centered versus variable-centered) impact support for various components of the Illness Identity model. Further, studies have generally focused on individuals with a broad range of levels of self-stigma; nevertheless, it is of great importance to study persons with high levels of self-stigma who are often the subject of targeted interventions.
The purpose of the present study, therefore, was to examine the relationship between self-stigma and variables found in the insight paradox and Illness Identity model in a group of people with schizophrenia-spectrum disorders with recently high levels of self-stigma. Specifically, the present study sought to test the predictions of the insight paradox using cluster analyses and multiple components of the Illness Identity model using path analysis. It was hypothesized that both analytic approaches would yield similar findings in support of the predictions of the Illness Identity model and the insight paradox.
Method
Data were drawn from wave 3 from a larger randomized controlled trial (RCT) of a self-stigma intervention conducted with persons meeting criteria for schizophrenia-spectrum disorders showing evidence of moderate to elevated self-stigma (see Yanos et al., 2019, for details on the RCT). An initial screening study was conducted first to identify persons with moderate to elevated self-stigma. The rationale for focusing on wave 3 data was that, at wave 1, there would be a restriction of range in self-stigma, as participants were specifically identified for the study based on the presence of elevated self-stigma. Likewise, at wave 2, data would be skewed toward lower self-stigma as this wave occurred immediately following clinical intervention targeting self-stigma. Wave 3 was expected to provide an opportunity to observe more variability in self-stigma while also allowing evaluation of its effects among persons who had previously had elevated self-stigma levels.
Procedure
Participants were recruited from 5 sites for both the screening study and the RCT: two partial hospitalization programs and one outpatient clinic in Newark and Piscataway, New Jersey, an outpatient program in Indianapolis, Indiana, and a VA Medical Center psychiatric rehabilitation program in Indianapolis. All sites serve persons meeting criteria for SMI with a majority meeting criteria for psychotic disorders. Trained research assistants (RAs) recruited participants from waiting rooms and community meetings at the program sites for the initial screening. Institutional Review Board approval was received from institutions with which investigators were affiliated, and all participants provided informed consent to participate in the research.
After providing informed consent, participants were screened with the Internalized Stigma of Mental Illness (ISMI) scale and a short demographic questionnaire. If participants exceeded a cutoff mean score of 1 (on a 0–3 scale) on the ISMI, RAs briefly described the overall project and, if participants indicated interest, arranged to meet to complete informed consent and the baseline interview.
At the baseline interview, RAs first administered the Structured Clinical Interview for DSM-IV (SCID-IV) to determine diagnostic eligibility (schizophrenia or schizoaffective disorder and lack of current substance dependence). Potential participants not meeting diagnostic criteria were excluded from further participation in the study.
Participants
One hundred and seventeen participants completed interviews at wave 3. Participants were predominantly male (n = 72; 61.5%), and predominantly African-American (n = 76; 65%) and European-American (n = 28; 23.9%), and primarily diagnosed with schizophrenia (n = 77; 65.8%) rather than schizoaffective disorder. Participants were typically in their mid-40’s (M = 47.3, SD = 11.7), with roughly a high school education (M = 12.1, SD = 2.4). Participant had typically been first hospitalized in their early 20’s (M = 23.8, SD = 9.8) and reported 9 prior hospitalizations on average, although the number of hospitalizations reported was quite variable (M = 9.1, SD = 13.7).
Measures
Diagnostic eligibility (diagnosis of schizophrenia/schizoaffective disorder and no current substance dependence) was assessed using the mood, psychotic, and substance use disorders modules the SCID-IV (Spitzer, Williams, Gibbon, & First, 1994), a commonly-used structured diagnostic interview.
Self-Stigma.
Self-stigma was assessed using the ISMI (Ritsher & Phelan, 2004; alpha = .88), a 29-item self-report measure, which presents participants with first person statements and asks them to rate them on a 4-point scale. Items are summed to provide five major scale scores: Alienation, Stereotype Endorsement, Discrimination Experience, Social Withdrawal and Stigma Resistance. Consistent with prior work (Brohan et al., 2010), we used the total score excluding the stigma resistance subscale, which tends to correlate poorly with the other subscales.
Self-esteem was assessed using the Rosenberg Self-Esteem Scale (RSES; Rosenberg, 1964; alpha = .73), a 10-item self-report scale. Hope was measured using the Beck Hopelessness Scale (BHS; Beck, Weisman, Lester, & Trexler, 1974) (alpha = .92), a 20-item self-report true/false measure (higher scores on this scale indicate less hope). Two dimensions of social functioning (interpersonal functioning and vocational functioning) were measured with the Quality of Life Scale (QLS; Heinrichs, Hanlon, & Carpenter, 1984), a 21-item rating scale administered via a semi-structured interview with four subscales: intrapsychic foundations (motivation and engagement), interpersonal relations (quality and quantity of interpersonal relationships), instrumental function (work, education and related activity), and commonplace objects and activities (participation in community-based activities). In keeping with the focus of the Illness Identity model on interpersonal and vocational functioning, current analyses focused on the interpersonal relations and instrumental function subscales of the QLS. Inter-rater reliability for audio recordings of interviews rated across sites was good to excellent, with intra-class correlations (ICCs) ranging from .82–.95. Psychiatric symptoms were measured using the Positive and Negative Syndrome Scale (PANSS; Kay, Fiszbein, & Opler, 1987), a 30-item clinician-rated measure evaluating positive symptoms, negative symptoms, and general psychopathology. For the present study we focused on 3 subscales five PANSS factors: positive symptoms, negative symptoms, and emotional discomfort (encompassing depression and anxiety). Inter-rater reliability for audio recordings of interviews rated across sites was good to excellent (ICCs ranging from .89–.94). Insight was measured using the G12 item from the PANSS. This item begins with the prompt “Do you think that you, at this time, have any psychiatric or mental problems?” and contains follow up questions regarding perceptions of the seriousness of the problem and the need for treatment. The item is then rated on a 1–7 scale from “absent” to “extreme.” The PANSS G-12 is one of the most common methods for assessing insight among people with SMI, and has been found to correlate highly (roughly .7) with other established methods of assessing insight, such as the Scale to Assess Unawareness of Mental Disorder (Michel et al., 2013).
Coping with symptoms was assessed using the Coping with Symptoms Checklist (CSC; Yanos, Knight, & Bremer, 2003), which assesses the use of coping strategies across five symptom areas including anxiety, depression, delusions, hallucinations, and mania. Participants who endorsed experiencing any of these symptoms on the PANSS were asked to indicate the frequency in which each strategy was used to manage the symptom in the past 2 weeks. Each domain contains strategies classified as problem-centered, avoidant, or neutral; responses across symptom domains were then summed and averaged into summary scores. For the present study, we focused on the avoidant coping subscale, consistent with the Illness Identity model’s focus on the relationship between self-stigma and avoidant coping. We found good internal consistency for the avoidant coping subscale (alpha = .87).
Statistical Analyses
Correlations between all study scales were initially examined. A cluster analyses was then conducted in SPSS 25 (using the K-means command) to examine groupings of participants based on both insight and self-stigma. A maximum-likelihood analysis determined that the optimal number of clusters was 3, with “fair” fit using the “silhouette measure of cohesion and separation” so 3 clusters were specified in the analyses. We then compared means between study variables between the 3 clusters using analysis of variance.
A path analysis was then conducted in Mplus version 8.4 to test the theoretical and causal relations between predictors of self-stigma and insight, and outcomes of positive and negative psychiatric symptoms using structural equation modeling (SEM). A multiple mediation model was constructed in which self-stigma and insight were considered exogenous variables and self-esteem, emotional discomfort, social avoidance, positive symptoms, and negative symptoms were considered endogenous variables. Within the model, self-esteem, emotional discomfort, and social avoidance were examined as mediators of the relationship between 1) self-stigma and insight and 2) positive and negative psychiatric symptoms because these factors may temporally precede or contribute to the experience of positive and negative symptoms. Three additional variables (i.e., avoidant coping, vocational functioning, and hopelessness) were originally included in the path model but were trimmed from the final model to maximize statistical power as they were not significantly associated with any other variables. Both the direct and indirect effects of self-stigma and insight were estimated in relation to positive and negative psychiatric symptoms. As a second step, a moderated mediation path model was constructed using the endogenous variables as mediators of the relationship between the moderator, the interaction of self-stigma and insight, and the outcome, positive and negative psychiatric symptoms (Edwards & Lambert, 2007; Hayes & Rockwood, 2017; Muthén & Muthén, 2017).
The path model was estimated using full information maximum likelihood (Muthén & Muthén, 2017). The chi-square test of model fit was used as a global measure of exact fit and the standardized root mean square residual (SRMR), root mean square error of approximation (RMSEA), the Tucker Lewis Index (TLI), and the comparative fit index (CFI) were used as measures of approximate model fit. However, in the identified model, all paths were estimated, which resulted in a saturated model whose fit indices were artificially perfect and, therefore, not interpreted. Standardized path coefficients were used to estimate significant (p < .05) pathways.
Results
Table 1 presents findings from correlations among study scales. As can be seen in Table 1, consistent with the predictions of the Illness Identity model, self-stigma was strongly inversely significantly correlated with self-esteem, and moderately significantly correlated with positive symptoms, emotional discomfort, and avoidant coping. Contrary to the predictions of the Illness Identity model, vocational and interpersonal functioning were not significantly associated with self-stigma. Lack of insight was only significantly associated with positive and negative symptoms, and negatively associated with interpersonal functioning. Of note, self-stigma and insight were essentially uncorrelated.
Table 1:
Means, Standard Deviations, and Inter-Correlations for Study Scales
| Variable (Range) | Mean (SD) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1.Self-Stigma (0–3) | 1.33 (.58) | --- | ||||||||
| 2. Self-Esteem (0–3) | 1.78 (.56) | −.65** | --- | |||||||
| 3. Hopelessness (0–1) | .41 (.31) | .13 | −.14 | --- | ||||||
| 4. Positive Symptoms (1–7) | 2.49 (1.01) | .26** | −.18 | −.06 | --- | |||||
| 5. Negative Symptoms (1–7) | 2.11 (.75) | .07 | .03 | .05 | .07 | --- | ||||
| 6. Emotional Discomfort (1–7) | 2.95 (1.13) | .47** | −.47** | .06 | .51** | .03 | --- | |||
| 7. Lack of Insight (1–7) | 3.06 (1.28) | .08 | −.08 | .12 | .43** | .42** | .10 | --- | ||
| 8. Avoidant Coping (0–3) | 1.41 (.46) | .38** | −.37** | .13 | −.09 | .03 | .27** | .01 | --- | |
| 9. Interpersonal Functioning (0–6) | 3.28 (1.36) | −.12 | .00 | −.19* | −.13 | −.57** | −.14 | −.38** | −.11 | --- |
| 10. Vocational Functioning (0–6) | 2.95 (1.07) | −.09 | .05 | −.01 | −.09 | −.18 | −.10 | −.05 | −.11 | .15 |
p < .01
Cluster Analysis
The cluster analysis yielded 3 clusters based on insight and self-stigma. The first cluster (N= 35) had high insight (M = 1.4, SD = .5) and low-moderate self-stigma (M = 1.23, SD = .53); the second cluster (N = 64) had moderate levels of insight (M = 3.5, SD = .5) and elevated self-stigma (M = 1.54, SD = .55); the third cluster (N = 18) had moderately low insight (M = 4.6, SD = .78) low self-stigma (M = .81, SD = .41). Based on the pattern in insight and self-stigma, we termed the groups high insight/low self-stigma, low insight/high self-stigma, and low insight/low self-stigma. Note that this combination of groups was different than what was found in Lysaker et al. (2007), in which a “high insight/high self-stigma” group was found. We then compared means in the study variables between the three clusters (see Table 2). As can be seen in Table 2, there was a significant difference between the groups in self-esteem, but the Tukey HSD revealed that the only significant difference was between cluster 3 (low insight/low self-stigma) and cluster 2 (low insight/high self-stigma), with participants in cluster 3 demonstrating significantly higher self-esteem. This indicates that, holding low insight relatively constant, self-stigma was the main driver of differences in self-esteem. For PANSS positive symptoms and interpersonal functioning, cluster 1 (high/low self-stigma) differed significantly from both other clusters, demonstrating lower positive symptoms and greater interpersonal functioning. This indicates that the combination of high insight and low-self-stigma was associated with both fewer symptoms and better interpersonal functioning, in comparison with both low insight groups (regardless of whether self-stigma was high or low). For PANSS negative symptoms, all groups differed from each other, with participants in cluster 1 demonstrating the fewest negative symptoms and participants in cluster 3 demonstrating the highest.
Table 2:
Mean Differences in Study Scales Between Clusters
| Cluster 1: High insight/Low self-stigma |
Cluster 2: Low insight/High self-stigma |
Cluster 3: Low insight/Low self-stigma |
|||||
|---|---|---|---|---|---|---|---|
| Variable (Range) | Mean (SD) | Mean (SD) | Mean (SD) | F | df | p | Tukey HSD |
| Self-Esteem (0–3) | 1.88 (.51) | 1.67 (.57) | 2.01 (.56) | 4.10 | 2, 114 | .02 | 2<3 |
| Hopelessness (0–1) | .33 (.31) | .46 (.30) | .39 (.35) | 1.82 | 2, 114 | .17 | |
| Positive Symptoms (1–7) | 1.97 (.65) | 2.68 (1.05) | 2.8 (1.1) | 7.4 | 2, 114 | <.01 | 1<2, 3 |
| Negative Symptoms (1–7) | 1.66 (.52) | 2.12 (.66) | 2.65 (.85) | 14.06 | 2, 114 | <.01 | 1<2<3 |
| Emotional Discomfort (1–7) | 2.8 (1.1) | 3.14 (1.15) | 2.56 (1.03) | 2.36 | 2, 114 | .1 | |
| Avoidant Coping (0–3) | 1.34 (.55) | 1.5 (.36) | 1.23 (.52) | 2.6 | 2, 95 | .08 | |
| Interpersonal Functioning (0–6) | 3.99 (1.35) | 3.13 (1.21) | 2.47 (1.26) | 9.68 | 2, 111 | <.01 | 1>2, 3 |
| Vocational Functioning (0–6) | 3.04 (1.17) | 3.00 (1.1) | 2.61 (.7) | 1.1 | 2, 111 | .34 |
Path Analysis
A path analysis was then conducted to examine self-stigma and insight as predictors of negative and positive symptoms, with self-esteem, emotional discomfort, and interpersonal relationships as potential mediators (see Figure 1). The path model accounted for between 17.1% and 42.9% of the variance in endogenous variable outcomes, indicating the model has practical significance. The model accounted for the highest proportion of variance in positive symptoms (42.9%), self-esteem (41.9%), and negative symptoms (37.7%), with a lower proportion of variance accounted for in emotional discomfort (27.0%) and social avoidance (17.1%). Results demonstrated relatively distinct pathways between 1) self-stigma and positive symptoms and 2) insight and negative symptoms. When examining the potential for a moderated mediation pathway, the interaction between self-stigma and lack of insight was not significantly associated with any direct or indirect paths. Findings provided no support for the hypothesis that self-stigma and insight interact to moderate related outcomes.
Figure 1.
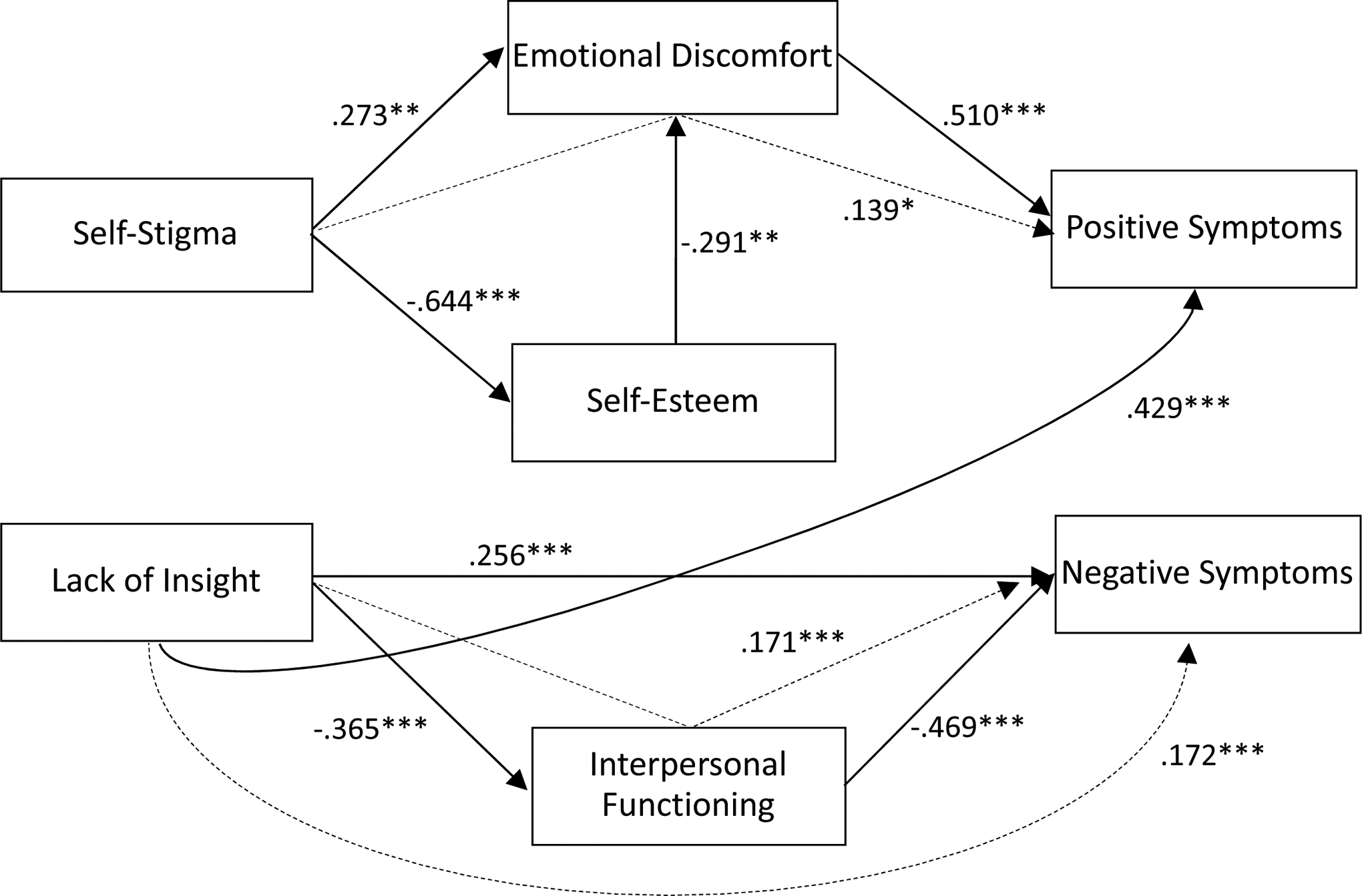
Path model examining self-stigma and insight as predictors of psychosocial function
Note. *p < .05. **p < .01. ***p < .001. Solid lines indicate direct paths. Dashed lines indicate indirect paths.
The direct paths between higher self-stigma and both lower self-esteem (B = −0.644, SE = .06, p < .001) and higher emotional discomfort (B = 0.273, SE = .10, p = .004) were significant. The direct path between higher emotional discomfort and more severe positive symptoms (B = 0.510, SE = .09, p < .001) was also significant. The total indirect path between higher self-stigma and greater positive psychiatric symptoms was not significant; however, examination of the specific indirect paths indicated the mediating role of emotional discomfort on the relationship between self-stigma and positive psychiatric symptoms (B = 0.139, SE = .06, p = .013).
The direct path between a higher lack of insight and worse interpersonal functioning (B = −0.365, SE = .08, p < .001), greater negative symptoms (B = 0.256, SE = .07, p < .001), and greater positive symptoms (B = 0.429, SE = .08, p < .001) were all significant. The direct path between better interpersonal functioning and less severe negative psychiatric symptoms (B = −0.469, SE = .08, p < .001) was also significant. Examination of specific indirect paths indicated the mediating role of interpersonal functioning on the relationship between insight and negative psychiatric symptoms (B = 0.171, SE = .05, p < .001). Although the total indirect path between lack of insight and greater negative symptoms was significant (B = 0.172, SE = .06, p < .001), the total set of variables accounted for little variance above and beyond the specific indirect association with social avoidance.
Discussion
In the current study, we sought to explore the relationship between self-stigma and components of the insight paradox and Illness Identity model using two different comprehensive analytic methods- cluster analysis and path analysis. Findings from the cluster analysis generally supported the predictions of the insight paradox, revealing that persons with both low self-stigma and high insight had less severe psychiatric symptoms and better interpersonal functioning than persons with both lower insight and greater self-stigma. Note that the cluster analysis did not produce a “high insight/high self-stigma” group which would have provided a more ideal contrast with the “high insight/low self-stigma” group.
Findings from the path analysis did not specifically support the insight paradox prediction, but indicated that both self-stigma and insight have separate relationships with outcomes related to recovery. Lack of support for the moderating effect of self-stigma may be partly explained by the pattern that can be observed in the cluster analysis- that, with the exception of self-esteem, low insight was generally associated with worse outcomes when self-stigma was both high and low, while high insight was only associated with positive outcomes when self-stigma was low. It may also be partly explained by differences in assumptions between person-centered analyses (which identify groups that share similar characteristics) and variable-centered analyses (which identify relationships between variables), which can sometimes lead to discrepant findings (Von Eye & Bogat, 2006). In the path analysis, generally consistent with the predictions of the Illness Identity model, self-stigma was found to be related to decreased self-esteem and increased emotional discomfort, and increased positive symptoms primarily through its relationship with emotional discomfort. At the same time, more impaired insight was found to be related to increased positive and negative symptoms. Results also indicated that, although insight was directly related to negative symptoms to a certain degree, it was also related to these symptoms through interpersonal functioning, hinting that higher levels of insight may facilitate increased interpersonal functioning, which may result in decreased negative symptoms.
There were some unexpected findings and not all aspects of the models tested were confirmed. Groups in the cluster analysis did not present significantly different levels of hopefulness. One possible explanation for this is that the clusters that emerged did not include a “high insight/high self-stigma” cluster that would have provided a clearer contrast to the “high insight/low-self-stigma” one. In fact, the emergence of a “low insight/high self-stigma” cluster (possibly persons who are ambivalent about the nature of their diagnosis and its implications), suggests that among persons with initially high self-stigma, insight and self-stigma may interact in more complex ways than previously demonstrated (e.g., Lysaker, Roe, & Yanos, 2007). The complexity of the nature of the relationship between insight and self-stigma was underscored by findings from a recent meta-analysis (Del Rosal et al., in press), which found no evidence for an overall relationship between self-stigma and insight. Additionally, a greater preference for avoidant coping, though correlated with higher levels of self-stigma in bivariate analyses, was not significantly associated with membership in any of the clusters (although correlational analysis indicated a relationship, and there was a non-significant trend for persons with low insight and high self-stigma to have a greater preference for avoidant coping). This may suggest that, among persons with initially high levels of self-stigma, coping and psychosocial functioning are related in more complex ways than found in other samples (e.g., Yanos et al., 2008). As with all unexpected and negative findings, however, replication and future research is needed before they are afforded significant weight. Interestingly, in both our analyses, findings converged to suggest that greater clinical insight may be related to healthier interpersonal relationships. This is consistent with a broad range of other literature that suggested that some awareness of psychiatric challenges may enable persons to form and sustain interpersonal relationships (Lysaker et al., 2018).
There were limitations. Our sample was restricted to people who had diagnosed with schizophrenia-spectrum disorders with initially high levels of self-stigma, after participating in a RCT of a stigma reduction intervention. Consequently, it is unclear whether the current results would generalize to others with high levels of self-stigma who are not in treatment, or who would decline to participate in this kind of treatment. It is plausible that exposure to clinical intervention may have weakened the link between insight, self-stigma, and outcomes predicted by the insight paradox, biasing findings. While we did not find differences in the proportion of persons in each cluster who received vs did not receive the active intervention, it cannot be known whether the active or control intervention affected the observed relationships.
A further limitation was reliance on a single measure of insight (the PANSS G12 item) that is biased toward a more traditional conceptualization of the insight construct (that is, the extent to which an individual agrees that they have a psychiatric disorder in need of treatment). Research indicates that measures of “narrative insight” (defined as the stories that people tell about their psychiatric experiences) overlap only moderately with traditional measures of insight, and do not differentiate between persons with a “passive acceptance” of their psychiatric label, and those with a more nuanced, integrative narrative understanding of their psychiatric experiences (Roe et al., 2008). A problem with measures of narrative insight is that they are much more time-consuming to assess than clinical insight, but this limitation should be addressed in future studies.
We also examined the relationships among variables at one time point only. Longitudinal research is needed to explore how these phenomena interact over time. For example, further analyses might examine whether baseline insight moderated the process of stigma change for participants receiving targeted anti-stigma intervention. To attain a testable path model and to maximize statistical power, the number of variables included had to be reduced. A post-hoc power analysis using the program GPower3.1.9.2 (Faul et al., 2007) found that this sample size had good power (1- β probability of greater than .95) to detect effects of R2 = .2 or greater, but weak power (1- β probability of greater than .65) to detect effects of R2 = .1 or lower. Limits in statistical power may partly explain why components of the Illness Identity model with weaker bivariate relationships (e.g., avoidant coping) were not able to be included in the path model. Future research testing the Illness Identity model should seek to use larger samples in order to detect more subtle effects between variables.
One clinical implication of our findings is that, at least among persons with initially high levels of self-stigma, there may be potential benefits to insight. They further suggest that interventions targeting self-stigma may be enhanced by a sensitivity to the importance of developing a nuanced understanding of one’s condition that may be consistent with the concept of “insight,” and that just reducing self-stigma in the absence of insight may have a more limited benefit.
Conflicts of Interest and Source of Funding:
The authors declare no conflicts of interest. Funding for this work was supported in part by grant R01MH0094310 from the National Institutes for Health.
Contributor Information
David Roe, University of Haifa
Paul H. Lysaker, Richard L Roudebush VA Medical Center and Indiana University School of Medicine
References
- Bamaca-Colbert MY, & Gayles JG (2010). Variable-centered and person-centered approaches to studying Mexican-Origin mother-daughter cultural orientation dissonance. Journal of Youth and Adolescence, 39, 1274–1292. 10.1007/s10964-009-9447-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck AT, Weisman A, Lester D, & Trexler L (1974). The measurement of pessimism: The hopelessness scale. Journal of Consulting and Clinical Psychology, 42, 861–865. 10.1037/h0037562 [DOI] [PubMed] [Google Scholar]
- Brohan E, Elgie R, Sartorius N, & Thornicroft G (2010). Self-stigma, empowerment and perceived discrimination among people with schizophrenia in 14 European countries: The GAMIAN-Europe study. Schizophrenia Research, 12, 232–238. 10.1016/j.schres.2010.02.1065 [DOI] [PubMed] [Google Scholar]
- Corrigan PW, & Watson AC (2002). The paradox of self-stigma and mental illness. Clinical Psychology: Science & Practice, 9, 35–53. 10.1093/clipsy.9.1.35 [DOI] [Google Scholar]
- Del Rosal E, Gonzalez-Sanguino C, Bestea S, Boyd J, & Munoz M (In Press). Correlates and consequences of internalized stigma assessed through the ISMI scale for people living with mental illness: A scoping review and meta-analysis from 2010. Stigma and Health. 10.1037/sah0000267 [DOI] [Google Scholar]
- Dubreucq J, Plasse J, & Franck N (2021). Self-stigma in serious mental illness: A systematic review of frequency, correlates, and consequences. Schizophrenia Bulletin, sbaa181. 10.1093/schbul/sbaa181 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Faul F, Erdfelder E, Lang A-G, & Buchner A (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavioural Research Methods, 39, 175–191. 10.3758/BF03193146 [DOI] [PubMed] [Google Scholar]
- Heinrichs DW, Hanlon TE, & Carpenter WT (1984). The Quality of Life Scale: An instrument for assessing the schizophrenic deficit syndrome. Schizophrenia Bulletin, 10, 388–396. 10.1093/schbul/10.3.388 [DOI] [PubMed] [Google Scholar]
- Kay S, Fiszbein A, & Opler L (1987). The Positive and Negative Syndrome Scale for Schizophrenia. Schizophrenia Bulletine, 13, 261–276. 10.1093/schbul/13.2.261 [DOI] [PubMed] [Google Scholar]
- Leamy M, Bird V, Le Boutillier C, Williams J, & Slade M (2011). Conceptual framework for personal recovery in mental health: Systematic review and narrative synthesis. British Journal of Psychiatry, 199, 445–452. 10.1192/bjp.bp.110.083733 [DOI] [PubMed] [Google Scholar]
- Livingston JD, & Boyd JE (2010). Correlates and consequences of internalized stigma for people living with mental illness: A systematic review and meta-analysis. Social Science and Medicine, 71, 2150–2161. 10.1016/j.socscimed.2010.09.030 [DOI] [PubMed] [Google Scholar]
- Lysaker PH, Roe D, & Yanos PT (2007). Toward understanding the insight paradox: Internalized stigma moderates the association between insight and social functioning, hope and self-esteem among people with schizophrenia spectrum disorders. Schizophrenia Bulletin, 33, 192–199. 10.1093/schbul/sbl016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lysaker PH, Pattison ML, Leonhardt BL, Phelps S, & Vohs JL (2018). Insight in schizophrenia spectrum disorders: a review of its relationship with behavior, mood and perceived quality of life, its underlying causes and emerging treatments. World Psychiatry, 17, 12–23. 10.1002/wps.20508 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michel P, Baumstarck P, Auquier P, Amador X, Dumas R, Fernandez J, Lancon C, & Boyer L (2013). Psychometric properties of the abbreviated version of the Scale to Assess Unawareness in Mental Disorder in schizophrenia. BMC Psychiatry, 13, 229. 10.1186/1471-244X-13-229 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muñoz M, Sanz M, Pérez-Santos E, de los Ángeles Quiroga M (2011). Proposal of a socio–cognitive–behavioral structural equation model of internalized stigma in people with severe and persistent mental illness. Psychiatry Research, 186, 402–408. 10.1016/j.psychres.2010.06.019. [DOI] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2017). Chapter 3: Regression and path analysis. In Muthén LK & Muthén BO (Eds.), Mplus user’s guide (8th ed., pp. 19–42). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Ritsher JB, & Phelan JC (2004). Internalized stigma predicts erosion of morale among psychiatric outpatients. Psychiatry Research, 129, 257–265. 10.1016/j.psychres.2004.08.003 [DOI] [PubMed] [Google Scholar]
- Roe D, Hasson-Ohayon I, Kravetz M, Yanos PT, & Lysaker P (2008). Call it a monster for lack of anything else: Narrative insight in psychosis. Journal of Nervous and Mental Disease, 196, 859–865. 10.1097/NMD.0b013e31818ec6e7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenberg M (1964). Society and the adolescent self-image. Princeton University Press. [Google Scholar]
- Spitzer RL, Williams JB, Gibbon M, & First M (1994). Structured Clinical Interview for DSM-IV. New York, NY: Biometrics Research. [Google Scholar]
- Von Eye A, & Bogat GA (2006). Person-oriented and variable-oriented research: Concepts, results and development. Merrill-Palmer Quarterly, 52, 390–420. https://www.jstor.org/stable/23096201 [Google Scholar]
- Yanos PT, DeLuca JS, Roe D, & Lysaker PH (2020). The impact of illness identity on recovery from severe mental illness: A review of the evidence. Psychiatry Research, 288, 112950. 10.1016/j.psychres.2020.112950 [DOI] [PubMed] [Google Scholar]
- Yanos PT, Knight EL, & Bremer L (2003). A new measure of coping with symptoms for use with persons diagnosed with severe mental illness. Psychiatric Rehabilitation Journal, 27, 168–176. 10.2975/27.2003.168.176. [DOI] [PubMed] [Google Scholar]
- Yanos PT, Lysaker PH, Silverstein SM, Vayshenker B, Gonzales L, West ML, & Roe D (2019). A randomized controlled-trial of treatment for self-stigma among persons diagnosed with schizophrenia-spectrum disorders. Social Psychiatry and Psychiatric Epidemiology, 54, 1363–1378. 10.1007/s00127-019-01702-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yanos PT, Roe D, Markus K, & Lysaker PH (2008). Pathways between internalized stigma and outcomes related to recovery in schizophrenia spectrum disorders. Psychiatric Services, 59, 1437–1442. 10.1176/appi.ps.59.12.1437 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yanos PT, Roe D, & Lysaker PH (2010). The impact of illness identity on recovery from severe mental illness. American Journal of Psychiatric Rehabilitation, 13, 73–93. 10.1080/15487761003756860 [DOI] [PMC free article] [PubMed] [Google Scholar]