
Figure 5.
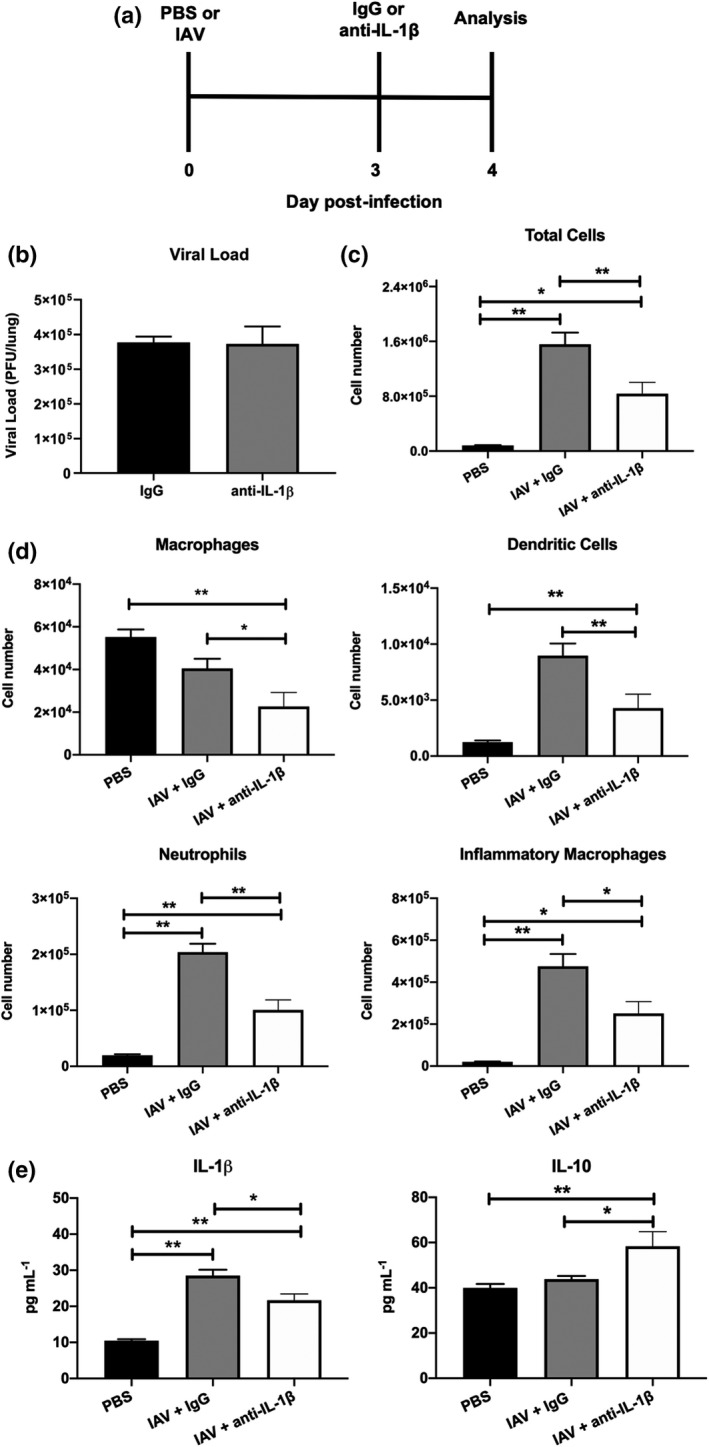
Anti‐IL‐1β antibody treatment modulates inflammation in the airways following IAV infection. (a–e) C57BL/6 mice were infected intranasally with 105 PFU of HKx31 (IAV). On day 3 postinfection, mice were intranasally treated with anti‐IL‐1β or control IgG antibodies. Control uninfected mice were treated with PBS alone (PBS). On day 4 postinfection (i.e. 24‐h postantibody treatment), parameters of disease were examined. (a) Experimental timeline. (b) Viral loads in the lung determined by plaque assay. Not significant; P > 0.05; Student’s t‐test. (c) Total numbers of cells in the BAL determined by viable cell count. (d) Numbers of Ly6G+ neutrophils, CD11c+I‐Abhigh dendritic cells, CD11c+I‐Ablow macrophages and Ly6C+ inflammatory macrophages in BAL determined by flow cytometry and viable cell counts. (e) Concentration of IL‐1β and anti‐inflammatory IL‐10 in BAL fluids determined by ELISA or cytometric bead array, respectively. (a–e) Data represent the mean ± s.e.m. Data from two independent experiments were pooled (n = 8). *P < 0.05, **P < 0.01; one‐way ANOVA. BAL, bronchoalveolar lavage; IAV, influenza A virus; IL, interleukin; PBS, phosphate‐buffered saline; PFU, plaque‐forming units.