
Figure 3. Figure showing the complexities of secondary prevention of atrial fibrillation (AF) with cardiac rehabilitation (CR).
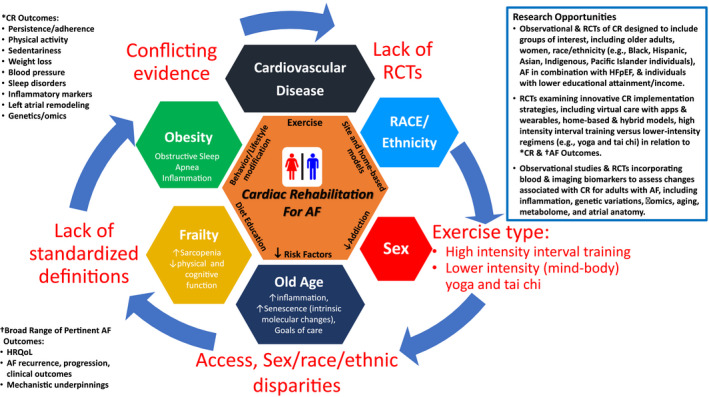
Inner hexagon: core components of CR include exercise training, risk factor reduction, education, lifestyle and behavior modification, and addiction curtailment (eg, alcohol and smoking), as well as new models of home‐based care that may all provide utility for AF, but specific benefits of multifaceted CR for AF remain poorly studied. Colored hexagons: (top to clockwise) depict some of the many issues that affect CR, and influence AF (eg, cardiovascular disease, race and ethnicity, sex, older age, frailty, and obesity). All remain poorly studied in relation to CR and AF. Red labels: (top to clockwise) depict some of the complex dynamics that factor into the limitations of contemporary CR research and clinical care.
- Lack of randomized controlled trials (RCTs) inclusive of diverse demographics, including sex, race, and ethnicity, as well as broader functional end points that may better reflect utility of CR for AF.
- Lack of precision in regard to exercise modes and intensities, with understanding of both physiological and behavioral implications that factor into CR for AF.
- Lack of inclusion of older adults with focus on related complexities of frailty, sarcopenia, cognitive changes, and intrinsic aging physiological features that may factor into particular benefits of CR for AF.
- Lack of inclusion of obese subgroups with distinctive behavioral, biological, and clinical challenges pertaining to CR for AF.
Black lettering (left top to clockwise) highlights some of the factors needed for improved AF research within CR:
- *Broad CR outcomes.
- †Broad range of pertinent AF outcomes.
- Research opportunities.
HFpEF indicates heart failure with preserved ejection fraction; and HRQoL, health‐related quality of life.