

Description
A 76-year-old woman presented with intermittent colicky left iliac fossa pain, diarrhoea and rectal bleeding. She denied of any weight loss, tenesmus and melaena.
Her medical history included gallstone pancreatitis and hypothyroidism. On examination, she had low-grade fever (37.8°C) and tenderness in the left iliac fossa. Investigations showed raised lactate (3.1 mmol/L), white cell count (25.2×109/L) and C reactive protein (196 mg/L). Stool culture was negative.
Her CT abdomen and pelvis showed diffuse oedema of the wall of descending colon (A) and a large intra-abdominal retroperitoneal fatty lesion with small calcifications in the left iliac fossa extending through inguinal canal (B) on figure 1.
Figure 1.

CT abdomen and pelvis (A) coronal view; (B) sagittal view.
Intravenous antibiotics and fluids were commenced but she still reported minor rectal bleeding. She remained haemodynamically stable and subsequently underwent flexible sigmoidoscopy which showed inflammation of the descending colon. The histology of descending colon obtained during flexible sigmoidoscopy showed neutrophils infiltrating the surface epithelium and congestion in the lamina propria (figure 2A). This was consistent with ischaemic colitis secondary to extrinsic compression by the fatty lesion (labelled B on CT abdomen and pelvis).
Figure 2.
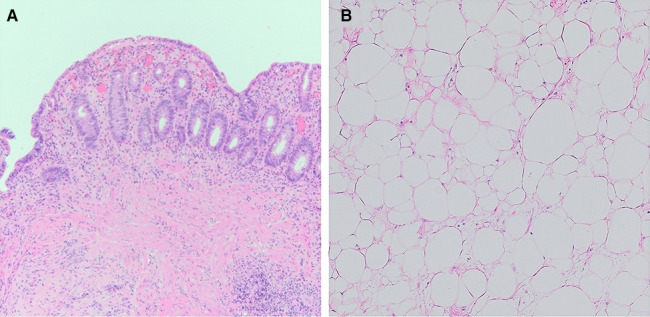
(A) Histology of distal descending colon. (B) Histology of retroperitoneal mass (labelled B on figure 1A, B).
After discussion at National Sarcoma Multidisciplinary Teams (MDT) meeting, she underwent laparotomy, excision of left retroperitoneal mass of 140 mm×70 mm×70 mm, en bloc left salpingo-oophorectomy and excision of thigh component of the mass. The biopsy of the retroperitoneal mass showed viable adipose tissue with scattered stromal nuclear atypia (figure 2B). This was consistent with the diagnosis of a well-differentiated retroperitoneal liposarcoma stage pT3, causing secondary ischaemic colitis.
Presentation with diarrhoea, colicky abdominal pain and mild rectal bleeding are common in both general medical and surgical admissions. Ischaemic colitis is not an uncommon cause for these presentations with an incidence of 22.9 cases per 100 000 person-years.1 Ischaemic colitis is commonly related to hypotension and cardiovascular diseases.1 However, it is also important for clinicians managing such patients to investigate for secondary causes of ischaemic colitis such as compression of vasculature by tumour, especially when there is not a clear history of hypotension preceding the event.
Soft-tissue sarcomas constitutes <1% of all malignancies with liposarcoma accounting for almost 40% of retroperitoneal sarcomas.2 Liposarcoma tends to be asymptomatic at the initial stage but can cause gastrointestinal problems due to compression of adjacent structures.2 However, we are unaware of any previous reports of it causing ischaemic colitis. This case highlights the importance of consideration of tumour as the cause of ischaemic colitis.
Learning points.
Soft-tissue sarcomas such as retroperitoneal liposarcomas are rare, but it can cause ischaemic colitis due to compression of the vasculature.
CT scan should be considered to rule out secondary causes of ischaemic colitis.
Footnotes
Contributors: TLG wrote the manuscript. TLG and IAM reviewed the literature. JL and RS analysed and provided the radiology and histology images. All authors edited the manuscript.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Ethics statements
Patient consent for publication
Consent obtained directly from patient(s).
References
- 1.Trotter JM, Hunt L, Peter MB. Ischaemic colitis. BMJ 2016;355:i6600. 10.1136/bmj.i6600 [DOI] [PubMed] [Google Scholar]
- 2.Tajudeen M, Dutta S, Bheemanathi S, et al. Pictorial essay on a case of giant retroperitoneal liposarcoma. BMJ Case Rep 2020;13. doi: 10.1136/bcr-2020-237607. [Epub ahead of print: 12 Dec 2020]. [DOI] [PMC free article] [PubMed] [Google Scholar]