
Figure 3.
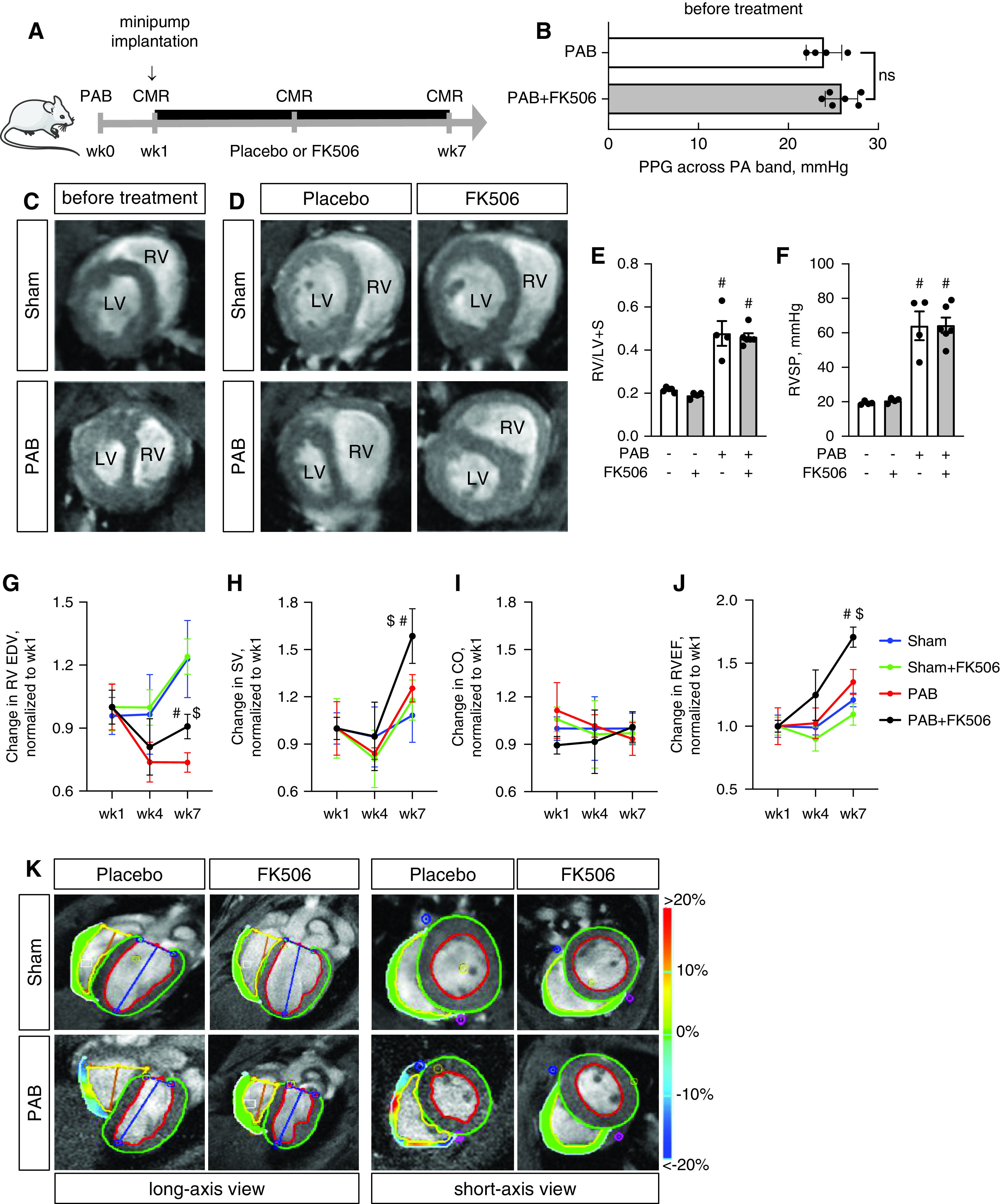
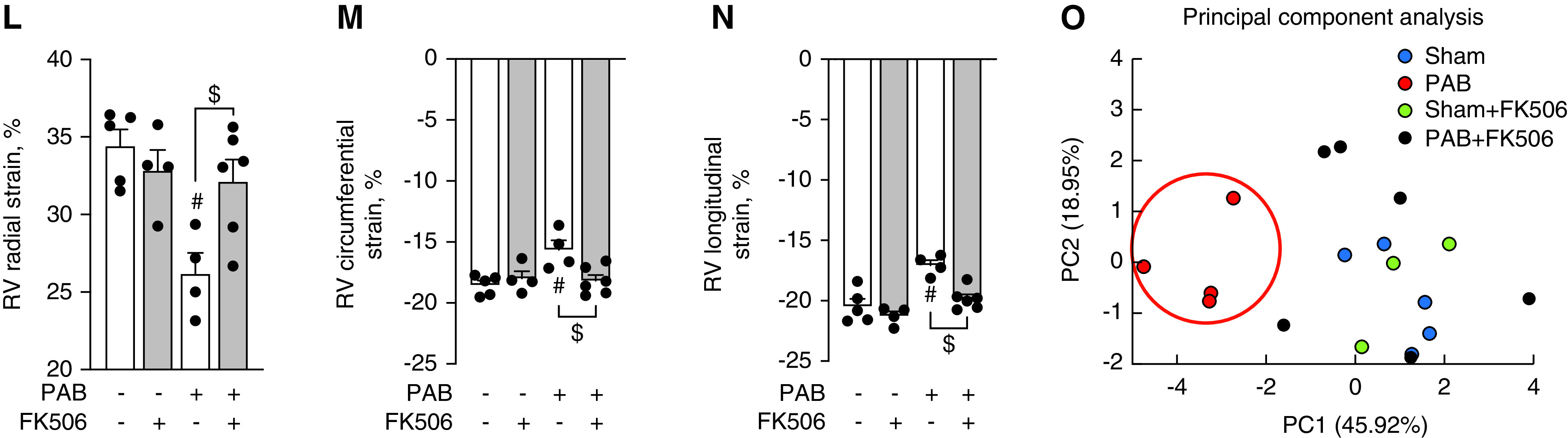
Treatment with FK506 improves RV function under chronic pressure overload conditions. (A) Male C57Bl6 mice underwent sham surgery or moderated PAB (around a 24-G needle) and received either placebo or FK506 (0.05 mg/kg/d via osmotic minipump) at week1 after surgery for additional 6 weeks. (B) Echocardiographic measurement of the PPG across the PA band before treatment commencement demonstrated a comparable degree of stenosis among both PAB groups. (C) CMR imaging confirmed hypertrophic RV remodeling 1 week after PAB. (D–F) FK506 therapy reduced septal flattening and compression of the left ventricle (LV) after PAB as compared with placebo control (D) without changes in RV free-wall hypertrophy, assessed via Fulton’s index (right ventricular [RV]/left ventricular [LV] + septal [S] weight) (E) or RVSP (F). (G–J) During the time course of pressure overload, FK506 attenuated the decrease in RV EDV (G) and increased RV SV (H), CO (I), and RVEF (J). (K–N) Strain imaging (K) further demonstrated increased RV deformation in radial (L), circumferential (M), and longitudinal (N) direction. (O) Principal component (PC) analysis was used to reduce 20 metrics of myocardial strain in both ventricles to three PCs, which showed that FK506-treated PAB animals cluster from placebo-treated PAB mice along PC1 scores, demonstrating that multiple indices of cardiac performance improve with FK506 treatment. n = 4–6 animals per group. Two-way ANOVA followed by Tukey’s multiple comparison post hoc analysis. #P < 0.05 versus sham. $P < 0.05 versus placebo. CMR = cardiac magnetic resonance; CO = cardiac output; EDV = end-diastolic volume; PA = pulmonary artery; PPG = peak pressure gradient; RVEF = RV ejection fraction; RVSP = RV systolic pressure; SV = stroke volume.