

Abstract
Rationale: For children with asthma, access to quick-relief medications is critical to minimizing morbidity and mortality. An innovative and practical approach to ensure access at school is to maintain a supply of stock albuterol that can be used by any student who experiences respiratory distress. To make this possible, state laws allowing for stock albuterol are needed to improve medication access.
Objectives: To provide policy recommendations and outline steps for passing and implementing stock albuterol laws.
Methods: We assembled a diverse stakeholder group and reviewed guidelines, literature, statutes, regulations, and implementation documents related to school-based medication access. Stakeholders were divided into two groups—legislation and implementation—on the basis of expertise. Each group met virtually to review documents and draft recommendations. Recommendations were compiled and revised in iterative remote meetings with all stakeholders.
Main Results: We offer several recommendations for crafting state legislation and facilitating program implementation. 1) Create a coalition of stakeholders to champion legislation and implement stock albuterol programs. The coalition should include school administrators, school nurses and health personnel, parents, or caregivers of children with asthma, pediatric primary care and subspecialty providers (e.g., pulmonologists/allergists), pharmacists, health department staff, and local/regional/national advocacy organizations. 2) Legislative components critical for effective implementation of stock albuterol programs include specifying that medication can be administered in good faith to any child in respiratory distress, establishing training requirements for school staff, providing immunity from civil liability for staff and prescribers, ensuring pharmacy laws allow prescriptions to be dispensed to schools, and suggesting inhalers with valved holding chambers/spacers for administration. 3) Select an experienced and committed legislator to sponsor legislation and guide revisions as needed during passage and implementation. This person should be from the majority party and serve on the legislature’s health or education committee. 4) Develop plans to disseminate legislation and regulations/policies to affected groups, including school administrators, school nurses, pharmacists, emergency responders, and primary/subspecialty clinicians. Periodically evaluate implementation effectiveness and need for adjustments.
Conclusions: Stock albuterol in schools is a safe, practical, and potentially life-saving option for children with asthma, whether asthma is diagnosed or undiagnosed, who lack access to their personal quick-relief medication. Legislation is imperative for aiding in the adoption and implementation of school stock albuterol policies, and key policy inclusions can lay the groundwork for success. Future work should focus on passing legislation in all states, implementing policy in schools, and evaluating the impact of such programs on academic and health outcomes.
Keywords: asthma, children, health policy, inhaler, medication
Contents
Introduction
Methods
-
Steps to Pass Stock Albuterol Legislation
Build Stakeholder Coalition
Create Issue Brief and Factsheets
Find a Legislative Sponsor
Address Opposition
Draft Legislation
Introduce Legislation
Testify
Passage of Legislation
-
Components for Implementation of Stock Albuterol
Policy Dissemination and Education
Training of School Personnel
Program Supplies
Standard Protocol for Medication Administration
Procedure for Event Documentation
Additional Considerations
Conclusions
Introduction
Asthma affects approximately 10% of school-aged children in the United States, with higher prevalence and morbidity being demonstrated among low-income and minority populations (1–4). Sixty percent of children experience an asthma exacerbation, leading to approximately 767,000 emergency department visits and 74,000 hospitalizations annually (1, 5). Compared with their peers, children with asthma miss more school days per year (6, 7), totaling 13.8 million absences annually (8).
School-aged children spend a majority of their day in school; therefore, evidence-based asthma care practices are important for guiding school asthma management (9–13). Guidelines recommend that all children with asthma have access to quick-relief medications. All 50 states and the District of Columbia permit children with asthma to self-carry and self-administer personal inhalers (14). However, access to emergency albuterol remains low, with studies suggesting that as few as 14% of children have quick-relief medication at school (15–17). Common barriers include difficulty accessing health care (18), challenges with obtaining asthma action plans and inhalers/valved holding chambers (VHCs) (15, 19–23), and the potential for lost or expired inhalers.
Because children with asthma may experience a sudden, unexpected, and life-threatening exacerbation at any time, access to albuterol can be life-saving. Although they are rare, there were a total of 192 asthma-related deaths among children in 2018 (1), and 38 asthma-related deaths occurred at school between 1990 and 2003 (24). Delays in albuterol administration were reported in one-third of these deaths, and a third of the delays were attributed to a lack of medication. Asthma-related deaths have also occurred among athletes on school sports teams, and up to 10% of high school athletes have undiagnosed asthma (25).
An innovative and practical mechanism exists to ensure that students with asthma have access to potentially life-saving quick-relief medication while at school. Schools, with the assistance of a medical consultant and appropriate training for staff (26), can make albuterol available to all students with, for example, a single albuterol inhaler that is used with a different VHC/spacer for each child. Although 88% of schools are willing to store students’ personal inhalers (27), few schools stock quick-relief medicine. A stock albuterol program ensures that a school has albuterol that can be used by any child experiencing respiratory distress. Expanding schools’ capacity to acquire and maintain stock albuterol may help maintain the safety of students with asthma when personal quick-relief medicines are unavailable, expired, or empty. Furthermore, when children lack a documented asthma diagnosis in school, access to quick-relief medicine may provide ready access to treatment for a student who has an established diagnosis but no documentation at school or a student with a first-time asthma episode.
Over the past decade, stock albuterol policies have increased across the United States, with at least 15 states passing such legislation and a few states with experience implementing such policies. One state reports that 84% of respiratory events treated with a stock inhaler resulted in the child returning to class (28, 29). Because these policies are relatively new, further data are not available on the impact of stock albuterol. Notably, the evidence shows that quick-relief medications are effective for respiratory distress and safe for children, thus demonstrating that access at school is important for improving outcomes. In light of students’ limited access to albuterol and the positive outcomes with stock albuterol, the goal of this statement is to advocate for stock albuterol legislation in all states and for wide-scale implementation to improve access to emergency asthma medications in schools.
Methods
We assembled a diverse group of stakeholders, including clinicians, pharmacists, researchers, policy experts, school nurses, and parents. Stakeholders included representatives from major organizations, including the American Thoracic Society, Allergy and Asthma Network, American Lung Association, and National Association of School Nurses. Conflicts of interest were collected from each stakeholder and vetted at the start of the project. Updates were requested throughout the project. No stakeholders had conflicts that required management during meetings and discussions. We applied our collective experience and expertise to develop this policy statement on stock albuterol legislation and implementation.
We first identified and reviewed guidelines, literature, statutes, and implementation documents related to school-based medication access. A literature search was conducted in the PubMed and Education Resources Information Center databases to identify existing literature about stock albuterol. Specific search terms included “albuterol,” “medicine,” “inhaler,” “nebulizer,” “stock,” “school,” “class,” “child,” and “student.” We examined relevant abstracts and conference programs to supplement this search. Our search focused specifically on the United States, given the differences among countries in terms of pharmaceutical and school-related regulation and legislation as well as the processes for passing and implementing policy. Because research in this area is limited, most information came from state statutes and implementation guides. Consideration was given to specific components of current policies, including the school type, medication indications, standing medical authority, training requirements, good faith use, and medical devices.
Stakeholders were divided into two groups—legislation and implementation—on the basis of expertise. Each group met two to three times virtually to review documents and draft recommendations. These recommendations were compiled and revised in iterative remote meetings with all stakeholders. On the basis of multiple data sources and expert opinions, we developed policy recommendations and outlined steps for passing and implementing stock albuterol laws.
Steps to Pass Stock Albuterol Legislation
Medical licensing, pharmaceutical drugs, and education are largely regulated at the state level; thus, legislation for programs like stock albuterol must occur within individual states. It is crucial to understand legislative processes and necessary steps to pass stock albuterol legislation within a state (Figure 1) (30, 31). The overall process is similar across states, and we review the basic steps below.
Figure 1.


Stock albuterol legislative steps. (A) The process for Senate bills. (B) The process for House bills. The process of passing a bill may differ across states and within the legislative chambers of a particular state (House and Senate). It is important to understand the process within your own state.
Build Stakeholder Coalition
The first step in passing stock albuterol legislation is to form a coalition of stakeholders (Table 1). Key stakeholders include healthcare professionals, school nurses, parents/guardians of children with asthma, pharmacy organizations, managed care organizations, advocacy groups, and legal groups, as well as health and education departments. Several key questions and pitfalls should be considered when building a stakeholder coalition (Table 2).
Table 1.
Key Stakeholders and Their Role in Stock Albuterol Legislation and Implementation
| Stakeholder Group | Examples | Expertise/Role in Legislation | Expertise/Role in Implementation |
|---|---|---|---|
| Nonprofit health organizations | • Allergy and Asthma Foundation of America | • Experience with legislative process | • Experience with implementation |
| • Allergy and Asthma Network | • State-specific knowledge | • Knowledge about legislation passed and relevant issues | |
| • American Academy of Pediatrics | • Relationships with specific legislators and stakeholders | • Develop and deliver training | |
| • American Lung Association | • Provide medical expertise, specifically on asthma | ||
| • American Thoracic Society | |||
| • National Association of School Nurses | |||
| • Asthma coalitions | |||
| • National professional medical, nursing, and pharmacy organizations | |||
| • State medical societies | |||
| School nursing | • National Association of School Nurses | • Understand how nurses are hired and function in schools | • Provide medical expertise, specifically on asthma |
| • National, state, and local organization representatives | • Provide expert testimony | • Share knowledge about legislation and relevant issues | |
| • State school nurse consultants | • Provide asthma and respiratory disease expertise | • Disseminate policy to school administrators/staff and children/families | |
| • School nursing leaders from districts | • Develop and deliver training | ||
| • Implement in schools | |||
| Healthcare professionals | • Primary care pediatricians | • Provide information on asthma and treating respiratory distress | • Write standing orders and prescriptions |
| • Asthma subspecialists (e.g., pulmonologists, allergists) | • Provide information on safety of albuterol | • Discuss policy with patients and families | |
| • Certified asthma educators | • Discuss training of lay personnel | ||
| • Academic researchers | |||
| Health and education departments | • State and/or county health department | • Ensure implementation considered in legislative process | • Disseminate policy broadly |
| • State superintendent | • Help support funding of program | ||
| • Board of Education | • Develop and deliver training | ||
| • School/district administration | |||
| School staff and administrators | • Principals/administrators | • Share insights about asthma care in school | • Understand and champion policy |
| • Teachers | |||
| • Coaches, security guards, and office clerks | • Participate in training | ||
| • Unions for teachers and staff | |||
| Healthcare organizations | • Managed care organizations | • Early awareness of legislation can facilitate implementation | • Provide avenue for potential funding |
| • State Medicaid Agency | |||
| • Private insurance companies | |||
| • Hospitals and emergency departments | |||
| Pharmacy | • State Board of Pharmacy | • State Board of Pharmacy should be part of legislation related to dispensing of medication to schools | • Provide medications and devices to schools |
| • Pediatric Pharmacy Association and other state and national pharmacy organizations | • National and state pharmacy organizations can support stock albuterol programs | • Communicate about drug recalls | |
| • Durable medical supply vendors | • Help communicate with pharmaceutical companies | ||
| Legal expertise | • Legislative counsel | • Consultation on appropriate legal language for drafting policy | • Support safe adoption of policy within school |
| • Trial Lawyers Association | • Children health policy expertise | ||
| Children with asthma and parents/guardians | • Elementary, middle, and high school students | • Provide personal stories and perspectives | • Raise awareness and champion policy |
| • Parents/guardians/caregivers | • Share stories of impact |
Listing does not indicate endorsement of document unless noted otherwise in statement.
Table 2.
Key Questions and Pitfalls in Building a Coalition of Stakeholders
| Building Coalition | Key Questions and Inclusions | Pitfalls to Avoid |
|---|---|---|
| Be clear about goals of engaging diverse stakeholders. | • How does engaging diverse stakeholders fit into your goals? | • Trying to engage people without clarity about goals |
| • What do you hope to achieve in short-term for legislation and long-term for implementation? | • Tokenistic approach in which focus is “getting people to the table” without commitment to authentic partnership and learning | |
| Invest in building relationships and trust. | • What types of relationships exist among different stakeholders? | • Narrow focus on “getting people to the table,” rather than partnership building |
| • What are ways to strengthen relationships and build trust? | • Paternalistic approach that does not recognize strengths | |
| • The goal is to engage diverse stakeholders early on to help future implementation efforts with due understanding of distinct perspectives and roles of each participant or group represented. | • Unwillingness to hear feedback that is not positive | |
| • Overlooking importance of relationship-building and focusing on tasks | ||
| • Focusing prematurely on formal structure of relationships | ||
| Recognize and work with different agendas and interests. | • What are priorities of different stakeholders you wish to engage? | • Assuming that coalition issues should be a priority for everyone or that people who do not engage are apathetic |
| • What are common interests? | • Allowing agendas of one group or few groups to dominate coalition | |
| • Can involvement in coalition add value for each stakeholder’s work or help them achieve goals? | ||
| • Do agendas of dominant groups within coalition get in way? | ||
| Explore different strategies for engaging communities. | • What are best strategies and structures to reach goals for engaging different stakeholders? | • Structuring coalition in a way that makes it difficult for groups with fewer resources to participate |
| • Are there other strategies that might meet your needs? | • Restricting engagement strategies to coalition building | |
| • How can momentum be maintained once legislation is passed but before implementation? | ||
| Build inclusive coalition culture. | • Are there barriers to participation built into coalition’s structure or how it conducts business? | • Making assumptions about how to be inclusive without talking to people you want to engage |
| • What type of coalition culture would be most welcoming and inclusive to diverse groups? | • Attachment to “right” way to do things, leaving no room for exploration | |
| Acknowledge and address differences in power and resources. | • How do differences in power and resources impact coalition and partnerships between groups? | • Ignoring differences in power and resources, and operating as if they do not exist |
| • What are ways to navigate differences and share power? | • Undervaluing the strengths of groups that have fewer resources | |
| • How can different groups in coalition share resources and strengths in a way that will benefit everyone? | • Bringing people to the table without sharing power | |
| • Are there ways to invest resources to build infrastructure and support participation of groups that have fewer resources? It is key to build infrastructure in the legislative process so that future implementation is successful. | • Allowing any group or clique to dominate the coalition |
Create Issue Brief and Factsheets
Next, an issue brief and factsheets should be developed and disseminated to summarize key asthma facts and policy considerations to help advocates garner support. These documents provide a framework and consistent message for discussions with legislators and testimony.
An issue brief is a two- to four-page summary of an identified problem with recommendations for solutions (see online supplement) (32).In the case of stock albuterol, this brief provides a concise summary of asthma prevalence, morbidity, and mortality; highlights state asthma-related policy; and describes similar legislation in other states. The brief also emphasizes how existing asthma state policies have affected change. If seeking an amendment to existing legislation (e.g., stock epinephrine for anaphylaxis), it is helpful to include any positive outcomes from that legislation.
A factsheet is a one-page document with a bulleted summary of facts relevant to the issue. This document provides a set of talking points for testimony and discussion; it can also be shared with legislators. Several organizations (e.g., the American Public Health Association) provide examples of pertinent factsheets for health-related policy issues, and states with existing stock albuterol policies have created topic relevant factsheets (see online supplement) (33).
Find a Legislative Sponsor
Concurrently, a legislator must be identified to sponsor the legislation. The sponsor’s background, experience, committee assignments, and political party can be critical to success. An ideal sponsor would have experience with education or public health issues (e.g., asthma, health disparities, health policy, school health), have sufficient time to devote to the issue, be a member of the majority party in the legislature (or House if control is split), and ideally be a member of a committee in which the bill could be introduced (e.g., the Health, Education, or Appropriations Committees). Lobbyists or coalition partners who advocate in the legislature have relationships with legislators and their staff and are important to include.
The first step is to connect with key staff of the legislator or committee through direct outreach via phone/e-mail or working through existing relationships of partners. Once a legislator agrees to sponsor stock albuterol legislation, it is critical to remain engaged to advance the process. Although staffing structures differ in every state’s legislature, staff must be treated with the same level of respect as the sponsor, given that staff remain in that role longer than some lawmakers are in office and are key to moving legislation forward. Regularly scheduled meetings and/or calls can be helpful, and frequency may depend on the legislative session length. Meetings may be held during an interim period between legislative sessions (often summer and/or fall) when preparatory writing occurs for the next session. The sponsor and staff can help advocates understand preliminary processes, which may include study sessions (to consider long-term issues), informational hearings (to introduce potential legislative topics), or sunrise processes (to outline the costs and benefits of proposed legislation) (34).
Address Opposition
To secure bill passage, it is essential to understand the arguments opposing part or all of the bill and effectively respond. Because opposition may emerge at various times, the understanding of opposition arguments and the development of responses need to be undertaken iteratively, starting as early as sponsor identification, as they may impact sponsorship decisions. The sponsor will need this information to effectively advocate for the bill. Policy staff on health and education committees in both legislative chambers (the House and Senate), advocacy organizations with legislative experience, and provider organizations can provide context about opposition and ways to overcome issues. Federal legislation can also support efforts to pass state legislation (see online supplement), and national stakeholders (e.g., healthcare and education associations) can influence state policy-makers. For stock albuterol, opposition may be raised regarding prescriptions for stock albuterol, persons who can receive stock albuterol (e.g., students vs. nonstudents, asthma diagnosis vs. no diagnosis), training personnel to deliver stock albuterol, and the safety of albuterol.
Draft Legislation
Before the legislative session, stakeholder meetings should occur to discuss key components to include in the legislation. Stakeholder organizations may assist with drafting or choose to use existing model policies (see online supplement) (32, 33). All 50 states have school stock epinephrine laws to treat anaphylaxis, and one strategy is to amend those laws to include stock albuterol. It is important to review how stock epinephrine laws have functioned and how stock albuterol may mirror or differ from epinephrine.
Key implementation principles should be considered early and incorporated into legislation to avoid future pitfalls. For example, consider the implementation burden on school nurses, such as staff training requirements for recognizing symptoms and administering medicine. School nurses champion the health and safety of students, and it is part of their duties to instruct in care for emergencies. Depending on state nurse practice acts, nursing delegation may be key, thus making direct training by the school nurse essential. Although we advocate for full-time nurses in every school, it is important to recognize that many schools do not have nurses or that nurses have limited time in the school building. Thus, legislation can incorporate online platforms or alternative mechanisms for training by school nurses, asthma educators, or other trained individuals; alternatively, this language can be included in committee reports or regulations developed after bill passage.
On the basis of states’ experiences to date, we created a list of essential and recommended components for stock albuterol legislation (Table 3). For example, schools should be allowed to use albuterol in respiratory emergencies, even when a child lacks a documented asthma diagnosis. Albuterol is a safe drug to administer to any child in respiratory distress (35–38). To obtain stock medication for schools/districts, pharmacy dispensing law(s) should also be addressed.
Table 3.
Essential and Suggested Components of Stock Albuterol Legislation
| Component | Explanation/Reasoning |
|---|---|
| Essential components | |
| Medication can be administered in good faith to any child in respiratory distress. | The bill should permit emergency use of stock albuterol for any student in respiratory distress, not only students known to have an asthma diagnosis. |
| Reasoning: | |
| • Many students have undiagnosed asthma and may have their first asthma exacerbation at school. | |
| • Emergency administration of albuterol may be necessary and time sensitive; review of records to determine whether a student has asthma may delay care. | |
| • There are few causes of respiratory distress in children that would not respond to or would be harmed by administration of albuterol. | |
| • Albuterol is a safe medicine. | |
| Establish training requirements for school staff. | The bill should outline details about how many staff should be trained and about how training should be conducted to ensure that enough staff have the necessary knowledge and skills to administer stock albuterol. |
| • The recommendation is that a minimum of two individuals be trained per school building at a ratio of one individual for every 225 students. | |
| • Recommend permitting live or remote training that can be accessed by school staff at a convenient time at no cost. | |
| Ensure immunity from civil liability for staff and prescribers. | The bill should provide: |
| • Immunity for medical professionals who write the orders as well as pharmacists who dispense orders. | |
| • Immunity for school districts, school staff, or agents of the school who have the required training and administer the albuterol in good faith. | |
| Ensure that pharmacy laws allow medication dispensing to schools. | In parallel with preparing legislation, review the state’s current pharmacy dispensing laws and assess whether it is necessary to update pharmacy state board laws. Specifically, it is important that pharmacies are able to dispense medication to a school/district rather than to a specific individual. |
| Suggested components | |
| Allow schools to accept donations of money or product. | Donations can help with financing for the implementation of stock albuterol programs. |
| Use metered-dose inhalers with VHCs/spacers. | Metered-dose inhalers with VHCs/spacers for administration of quick-relief medication allows for the inhaler to be used for multiple individuals with less cleaning, easier storage/portability, and reduced aerosolization of particles. |
| Ensure authorization of parents or caregivers/school volunteers to administer albuterol. | Include parents or caregivers as well as school volunteers as authorized administrators of stock albuterol to ensure that they are indemnified from good faith use if they have appropriate training. |
| • There are many situations in which parents or caregivers as well as school volunteers act as agents of the school, such as during after-school activities, field trips, and sports. | |
| Ensure inclusion of nonpublic schools (e.g., private, tribal). | States often do not have significant oversight for activities in nonpublic (e.g., private, tribal) schools, as they are not state licensed. |
| • Stakeholders should explore state-specific strategies with legislators to include nonpublic schools in legislation. | |
| • Even if a school does not fall under state licensing requirements, prescribing providers and dispensing pharmacists need to legally be able to provide stock albuterol for nonpublic schools. |
Definition of abbreviation: VHC = valved holding chamber.
Legislation drafts should be shared with stakeholders to negotiate compromises to any key concerns. It also may be important to reach out to the state governor’s office while drafting legislation, as this office may provide feedback to incorporate into the bill. Engaging these groups early to discuss concerns helps move the bill smoothly toward passage and minimize the potential of a delay or veto.
Before bill introduction, costs incurred by the state must be estimated through a fiscal note produced by the legislature. Most state legislation has allowed, but not required, schools to stock albuterol. The reason is that funding for such policies is difficult to obtain, and as such, legislation is less likely to be passed if funding is required. Many stakeholders are not supportive of unfunded school mandates because it puts undue burden on already underfunded schools.
Introduce Legislation
Each state has different processes for introducing and passing legislation. The state legislature’s website provides legislative session details, including the state’s processes and timelines for introducing legislation. Formal introduction typically occurs when the legislative session starts, although some states start work on bills earlier and have deadlines after which legislation can no longer be introduced.
Legislation can be introduced in one or both houses of the legislature. The strategy around advancing legislation, including whether to introduce in one or both houses, is typically decided by the coalition supporting the legislation and the legislative sponsor. States have 1- or 2-year sessions. Typically, if a bill is not acted on in a state within the first year of a 2-year session, it will carry over to the session’s second year. Details of how a bill moves through the House and/or Senate are depicted in Figure 1.
Testify
It is important to identify key people to testify in support of the legislation and understand how testimony occurs. The speaker must register in advance so that they are called on during the bill’s hearing. The statement should begin with the proper address and thank you to the bill sponsor. For example, an opening could be “Chair and senators, thank you for allowing me to testify on an issue that is of extreme importance for the safety of our school children.” Testimony is usually limited to 1–2 minutes, prompting most individuals to prepare a script. Testimony should end with an “ask,” such as, “Therefore, I would urge you to vote “yes” to Bill [number] allowing schools to stock albuterol medication for respiratory emergencies.” After each testimony, legislators can ask questions.
Different stakeholders bring important expertise and experience for testimony (see online supplement). Clinicians can speak about asthma prevalence, symptom frequency, and safe treatment of respiratory episodes with albuterol. Common questions include “What happens if albuterol is given to children who do not have asthma?” and “What are side effects of albuterol?” We suggest that the testimony include several points: it should be noted that if the school calls 911, it is likely the child will receive albuterol from emergency responders; it should be noted that it is better for a child to be given albuterol as a potentially life-saving medication than for treatment to be withheld, which would increase the risk of poor outcomes; and it is also important to discuss the safety profile of albuterol across a range of doses (34). In addition, school nurses can discuss how difficult it is to obtain a child’s asthma medications for school, care for children with respiratory distress in a nonhealthcare setting, and reach parent/guardians. They can discuss how availability of stock albuterol would allow treatment to begin while awaiting emergency assistance (39). Most school nurses have experienced caring for students during a respiratory emergency, and without albuterol, the only option is to call parents/guardians and/or 911. This treatment delay can be difficult when albuterol may allow a child to return to class or may lessen the severity of symptoms. Finally, a school-aged child with asthma or their parent/guardian can share a story of a respiratory episode without available albuterol.
Passage of Legislation
Proposed legislation is discussed and voted on in committee and then on the floor in each chamber. Revisions to the legislation may occur at each step. The timeline for voting in each chamber depends on the legislators who control the floor schedule. Once both chambers pass the legislation, it is acted on by the state governor, and this action includes signing it or vetoing it. If signed by the governor, the legislation is enacted as a law. If the legislation is vetoed, the state legislature can override the veto, usually with a supermajority vote (e.g., two-thirds of legislators).
Components for Implementation of Stock Albuterol
Once legislation is passed, regulations are developed by designated state agencies (e.g., the board of education, health department). Then, efforts must be directed to implementation. Schools should be prepared to complete several steps for successful implementation (Figure2) (40). Although processes may differ across schools/districts, it is critical to engage stakeholders in key components to successfully implement stock albuterol (Table 1). Importantly, it should be recognized that stock albuterol is one piece of asthma care within the school, which should include education for affected students, training for staff, access to medications, and more.
Figure 2.
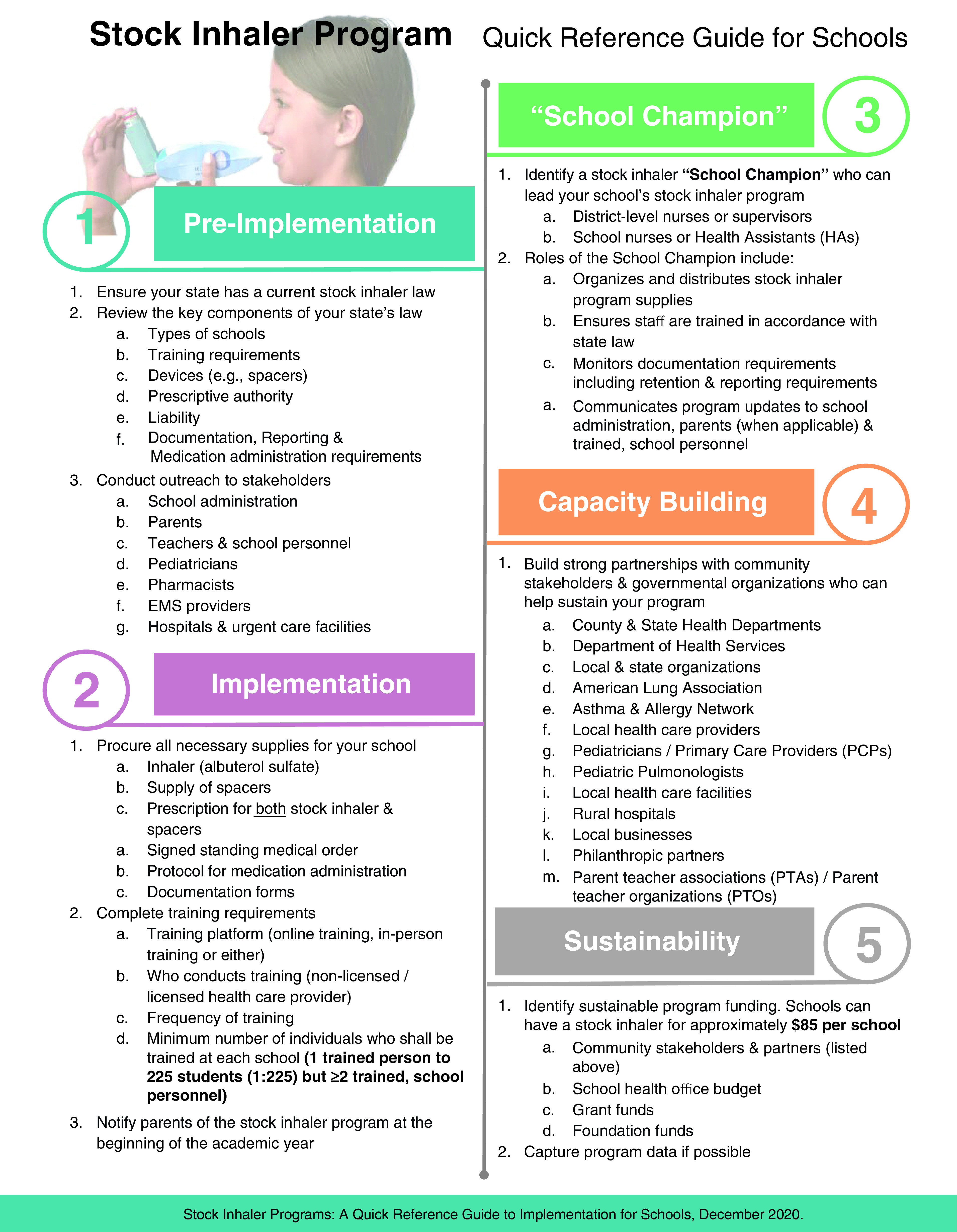
Stock albuterol program: quick reference guide for schools. Reprinted by permission from Reference 40.
Policy Dissemination and Education
Stock albuterol policy must be broadly disseminated. State-level professional organizations and advocacy groups are useful dissemination avenues for healthcare professionals (e.g., prescribers, nurses, pharmacists). Local and state-level health departments, education agencies, or policy e-mail listservs can serve as additional channels to disseminate policy and provide sample wording for school/district-level policies. School/district-level administrators and medical directors/nurses should notify school personnel about the policy.
Families and students are essential to effectively implementing stock albuterol policy. Annual notification about the policy should be sent home to families. To minimize barriers to life-saving medication, the policy should not require parents/guardians to sign waivers allowing albuterol administration in an emergency. Ideally, the policy should specify that school staff can assume parent/guardian consent in the case of emergency medications. Communication should be provided about by whom, when, and how medication will be administered, maintained, and stored and also about how staff will be trained. Parents/guardians must know stock albuterol does not replace the need for children to have their own quick-relief medications. A parent/guardian champion may be helpful for garnering support within the school community.
Training of School Personnel
To effectively implement the policy, annual training is critical to ensuring requisite knowledge and skills of school personnel who are designated to administer stock albuterol for respiratory symptoms or a respiratory emergency. At each school, a minimum of two individuals should be trained per building, with consideration given to additional individuals on the basis of asthma prevalence and other school indicators (e.g., population, social needs) (41). It is preferable to train as many as feasible to ensure that at least one trained individual is present in school daily. Both licensed and unlicensed school personnel, including unlicensed assistive personnel, may be designated to administer stock albuterol. Training should be geared to both groups, regardless of experience, in alignment with state legislation.
Training content about stock albuterol for school staff should include 1) signs and symptoms of respiratory distress; 2) an overview of asthma medications that includes inhaler administration, technique, maintenance, and cleaning; and 3) a protocol to manage respiratory episodes. Opportunities to teach back are particularly important to ensuring proper technique. Training should be delivered by individuals with requisite knowledge and expertise in asthma and stock albuterol policy. School nurses are key professionals who can provide and/or facilitate training on stock albuterol for school personnel. Partnerships with local organizations and/or coalitions (e.g., the American Lung Association, Allergy and Asthma Network) are also encouraged.
Content may be delivered synchronously or asynchronously with in-person or remote (e.g., web-based, video) methods. In-person workshops are ideal for school personnel with limited prior health experience or who prefer hands-on learning, especially for reviewing inhaler techniques for which immediate feedback is beneficial. In contrast, a standardized web or video-based curriculum provides flexibility, as many schools are unable to hold training that can be attended by all designated personnel. Because schools typically experience cyclic transitions of personnel throughout the academic year, flexible training options are necessary.
Program Supplies
Stocking albuterol in schools requires annual funding, primarily for supplies, for effective implementation. Essential program supplies are reported in Table 4 (see also the online supplement). To enable each school/district to meet its unique needs, policy should specify flexible options to procure supplies and promote equity for all students in the state, regardless of resources within a school or district.
Table 4.
Essential Components to Implement Stock Albuterol in Schools
| Essential Component | Explanation/Reasoning |
|---|---|
| Dissemination and education about policy | After legislation is passed, it is critical to broadly disseminate the policy to healthcare providers, school staff, and families. It is also important to provide annual education and communication about the legislation. Key individuals who should be involved in dissemination and education about the policy include: |
| |
| Training | At each school, a minimum of two individuals should be trained per building at a ratio of one trained individual for every 225 students. |
| School nurses are key professionals who can provide and/or facilitate training of school personnel on stock albuterol. Training should include: | |
|
|
| Orders and prescriptions | Key supplies needed for stock albuterol program (with cost*) include: |
| |
| A standing medical order and/or prescriptions are needed to obtain albuterol and valved holding chambers/spacers for each school. | |
| Supplies | Program supplies require funding of <$85 for a stock inhaler and needed materials for a school. Program expenses may vary on the basis of student enrollment, the school layout, and the community asthma prevalence. Schools with a large student body, sports programs, or extracurricular activities may opt to purchase additional stock albuterol inhalers to store in convenient locations (e.g., the gym, fields). |
| Standardized protocol | The protocol provides instructions regarding the use of stock albuterol in case of respiratory distress. It should include: |
| |
| Documents | Schools need the following forms for the implementation of stock albuterol: |
|
Cost is based on 2020 dollars.
Ideally, schools can procure supplies by using the school health annual budget. Alternative mechanisms include product or monetary donations from interested organizations (e.g., pharmaceutical companies, patient advocacy groups, hospitals), discounts or reimbursements from pharmaceutical companies, or fundraising through existing stakeholders, such as parent–teacher groups. Current programs cost less than $85.00 (in 2020 dollars) for an albuterol inhaler and needed supplies for a school (29). Program expenses may be affected by the number of inhalers needed at the school. We recommend at least one quick-relief inhaler per school building, with additional inhalers being added on the basis of student enrollment, the school layout (e.g., the number of buildings, locations of playgrounds and fields), and asthma prevalence.
Albuterol may come from pharmacies, pharmaceutical companies, or manufacturers. School nurses or medical directors should keep records of where medication is obtained and contact information if product issues arise. They should also monitor national databases for drug recalls (42). If the school uses a pharmacy to obtain albuterol, it is beneficial to develop relationships with the pharmacy manager to ensure notification of a drug recall or shortage.
In the school, stock albuterol should be stored in a temperate, dry, and unlocked place that is easily accessible to trained individuals for medication administration. Medication expiration dates should be monitored. All medications should be disposed of on the basis of school procedures.
Metered-dose inhalers (MDIs) should be primed before administration and cleaned after each use, as per manufacturer instructions (e.g., before the first dose, if not used for 2 wk). The MDI should always be used in conjunction with a one-way VHC/spacer ($3–$6 per unit). Most VHCs/spacers are constructed of plastic, but they are also available in cardboard models. The plastic models are available in rigid and collapsible versions and tend to be more expensive. Cardboard VHCs/spacers are also collapsible and relatively less expensive. Plastic and cardboard VHCs are equally effective, not suitable for use by more than one child, and should be cleaned or stored as per the manufacturer instructions. Schools can stock a supply of VHCs/spacers and use one per child, while using a single MDI. Once a child uses a VHC/spacer (plastic or cardboard), it should be stored in its original packaging and labeled with the child’s name if reuse is needed later during the school year, as studies show paperboard spacers can safely last the entire school year without microbial growth (43).
Standardized Protocol for Medication Administration
Every school should follow a standardized protocol for stock albuterol administration that is created and adopted at the school, district, or potentially state level and aligns with school, nursing, and other relevant regulations. The protocol should include specifics about who can receive medicine, what symptoms warrant albuterol, the number of doses to administer, how to assess the response, when to repeat administration, and what to do if medication is or is not effective.
Schools/districts in states that lack a standardized protocol should identify a medical consultant (or prescriber authority) to work with them to implement an existing or modified protocol that can be widely adopted. Medical consultants who sign the standing medical order should have the ability to modify existing protocols on the basis of their clinical practice and guideline-based care. For example, in Arizona, a protocol using a standardized number of inhaler actuations (instead of a dose range) stratified by the initial presentation of symptoms was widely adopted (29). Importantly, treatment for any child who requires stock albuterol should follow the standardized protocol and prescription instructions specified on the standing medical order, regardless of whether they have an asthma action plan on file at school. An asthma action plan provides school personnel with instructions on how to use a child’s personal medicine, not stock albuterol.
Procedures for Event Documentation
All respiratory episodes requiring stock albuterol should be documented by trained school personnel (Table 5). Documentation should be retained on file with the school in accordance with school policy for student health information as well as state legislation and regulation for stock albuterol. For states that have adopted stock epinephrine in schools, these procedures can be adapted to document stock albuterol administration.
Table 5.
Data Elements for Documentation of Stock Albuterol Usage Event Reporting in Schools
| Description | Data Element |
|---|---|
| Date | Date the event occurred |
| Time | Time of d the event occurred |
| Responding person | Fill-in-the-blank space for name and role |
| Student’s or individual’s name | First name |
| Last name | |
| Student’s or individual’s age or date of birth | Fill-in-the-blank space |
| Student’s or individual’s gender | Male |
| Female | |
| Nonbinary | |
| Student’s or individual’s race | American Indian or Alaska Native |
| Asian | |
| Black or African American | |
| Native Hawaiian or Pacific Islander | |
| White | |
| Multiracial | |
| Student’s or individual’s ethnicity | Hispanic or Latino |
| Non-Hispanic or non-Latino | |
| Previously known asthma diagnosis | Yes |
| No | |
| Unknown | |
| Reason for stock albuterol use (e.g., symptoms) | Fill-in-the-blank space |
| Number of inhaler actuations (e.g., puffs) | Checkboxes for number of puffs based on protocol; also provide option for off-protocol with blank for number puffs and reason |
| Student or individual’s disposition status | Returned to class |
| Sent home | |
| Summoned EMS and not transported | |
| Summoned EMS and transported | |
| Contact with parent/guardian | Open-ended |
| Comments (e.g., why stock albuterol inhaler was used) | Open-ended |
Definition of abbreviation: EMS = emergency medical services.
Additional information can be recorded at the school level or individual level, including the national drug code and lot number of the albuterol medication.
States with existing infrastructure can assist schools with maintaining documentation of quick-relief medication through centralized databases with medication events for epinephrine, naloxone, and albuterol. However, many states do not have infrastructure capable of systematic data collection on medication administration in schools. In this scenario, schools should create a documentation system that reports events in both the child’s individual health record and a centralized place (within the school or electronically) for all stock albuterol events that occurred during a single academic year. Procedures should be reviewed annually.
Together with documentation, parents/guardians should be notified each time their child uses stock albuterol to encourage follow-up with their primary care or subspecialty clinician and to obtain an inhaler to have at school. Frequent communication among the school, family, and medical home should occur, especially for children who use stock albuterol more than once in a school year. If a child does not have an asthma diagnosis, the family should be advised to follow up with a healthcare professional to be evaluated for asthma, and, if necessary, a referral should be made. Template communication resources are available (see online supplement).
Additional Considerations
Children and/or adults.
Traditionally, emergency use protects both children and adults with emergency needs. For stock albuterol, the legislation varies by state in terms of whether only children or anyone is included. Approximately half of the 15 states with stock albuterol legislation include adults, representing a gap that should be considered in future legislation and in amendments to current policies.
Stock inhaler versus nebulizer.
Several states allow administration of stock albuterol via an inhaler and/or nebulizer, although specific policies vary by state in terms of which of these can be administered by school nurses or designated personnel. The literature shows that MDIs with VHCs/spacers are as, if not more, effective than nebulizers in children during acute respiratory episodes (44). Stock nebulizers also have greater upfront cost, although the cost of albuterol used in nebulizers is presently less expensive than an inhaler; this may change as generic quick-relief inhalers become more available. Nebulizer machines are bulky and lack portability, making them less practical in certain situations (e.g., recess, before exercise). Although the administration of medicine through nebulizers tends to be easier, it takes longer to administer the same dose when using nebulizers, keeping students out of class longer. On balance, we recommend inhalers with VHCs/spacers as the preferred stock albuterol delivery system in schools, unless otherwise clinically indicated.
Stock albuterol and coronavirus disease.
The severe acute respiratory syndrome coronavirus 2 pandemic has changed practices around albuterol administration via nebulizers. Nebulizers are not recommended in school settings during the pandemic because of the potential for the spread infectious aerosols. Instead, stock albuterol MDIs can be used when they are properly cleaned after use with a single, one-way VHC/spacer for each child. As per CDC guidance, proper personal protective equipment should be used by the staff person aiding in any inhaled or nebulized medication administration, and medicine should not be administered in the classroom with other children present (45).
Conclusions
Because albuterol is a safe and potentially life-saving medication that is recommended by guidelines, it is important that schools make quick-relief medications available to all school-aged children, both with and without a documented asthma diagnosis. This failsafe measure can prevent exacerbations, reduce emergency service calls to schools, and enable children to return to class (29). Stock albuterol legislation is imperative to aiding in adoption and implementation, and key policy inclusions can lay the groundwork for success. A strong group of stakeholders and a carefully chosen sponsor are crucial to successful legislation and implementation across the United States. Future work should focus on passing legislation in all states and implementing policy in schools as well as on evaluating the impact of such programs on academic and health outcomes. Effective implementation of stock albuterol can help ensure that children have access to medication that enables them to live, learn, and play.
Acknowledgments
This official policy statement was prepared by an ad hoc task force of the American Thoracic Society, Allergy and Asthma Network, American Lung Association, and National Association of School Nurses.
Members of the task force are as follows:
Anna Volerman, M.D. (Co-Chair)1,2*‡
Ashley A. Lowe, Ph.D., M.S.P.H. (Co-Chair)3*‡
Lynn B. Gerald, Ph.D., M.S.P.H. (Co-Chair)3*
Charmayne M. C. Anderson, M.P.A.4
Kathryn V. Blake, Pharm.D.5
Tyra Bryant-Stephens, M.D.6
Thomas Carr, B.A.7
Heather Carter, Ed.D.8§
Lisa Cicutto, R.N., A.C.N.P., Ph.D.9
Joe K. Gerald, M.D., Ph.D.10
Jamila Jefferson, B.S., M.S.N., R.N., C.S.N.11‖¶
Tina Miller, B.S.N., R.N., N.C.S.N.12¶
Nuala S. Moore, M.A.13
Andrea A. Pappalardo, M.D.14,15*‡
Hanna Phan, Pharm.D.16
S. Christy Sadreameli, M.D., M.H.S.17
Andrea Tanner, M.S.N., R.N., N.C.S.N.18
Tonya A. Winders, M.B.A.4
*Subgroup leader.
‡Co–first author.
§Former Arizona State Senator.
‖Member of the task force who was not part of the writing committee.
¶School nurse.
1Department of Medicine and 2Department of Pediatrics, University of Chicago, Chicago, Illinois; 3Department of Health Promotion Sciences, 8Arizona Center for Rural Health, Mel and Enid Zuckerman College of Public Health, and 10Community, Environment, and Policy Department, University of Arizona, Tucson, Arizona; 4Allergy and Asthma Network, Vienna, Virginia; 5Nemours Center for Pharmacogenomics and Translational Research, Nemours Children’s Health System, Orlando, Florida; 6Community Asthma Prevention Program, Children’s Hospital of Philadelphia, Philadelphia, Pennsylvania; 7American Lung Association, Chicago, Illinois; 9Department of Medicine, National Jewish Health and University of Colorado, Denver, Colorado; 11The School District of Philadelphia, Philadelphia, Pennsylvania; 12Clark County School District, Las Vegas, Nevada; 13American Thoracic Society, Washington, DC; 14Department of Medicine and 15Department of Pediatrics, University of Illinois at Chicago, Chicago, Illinois; 16Department of Clinical Pharmacy, College of Pharmacy, C. S. Mott Children’s Hospital and University of Michigan, Ann Arbor, Michigan; 17Department of Pediatrics, Eudowood Division of Pediatric Respiratory Sciences, Johns Hopkins University, Baltimore, Maryland; and 18School of Nursing, Indiana University, Indianapolis, Indiana
Acknowledgment
The authors thank Rachel Abraham and Kayleigh Lawson-Michod, both M.P.H. graduates in Health Policy at the University of Arizona, for creating the figures. They also thank Jamila Jefferson for thoughtful insights provided for the development of this statement.
Footnotes
Endorsed by the Pediatric Pharmacy Association June 2021.
This document has an online supplement, which is accessible from this issue’s table of contents at www.atsjournals.org.
Author Disclosures: A.V. served on an advisory committee for Chicago Asthma Consortium; and received research support from ATS Foundation, CHEST Foundation, Health Resources and Services Administration, National Heart, Lung, and Blood Institute, National Institutes of Health, and Robert Wood Johnson Foundation. L.B.G. received research support from Thayer Medical. T.C. is an employee of the American Lung Association. L.C. received research support from the Colorado Department of Public Health and Environment, and the National Institutes of Health. A.A.P. served on an advisory committee for Chicago Asthma Consortium; served as a consultant for OptumRx/UnitedHealth Group; and received research support from the FARE Discovery Network. A.A.L., C.M.C.A., K.V.B., T.B.-S., H.C., J.K.G., J.J., T.M., N.S.M., H.P., S.C.S., A.T., and T.A.W. reported no commercial or relevant noncommercial interests.
Contributor Information
Collaborators: on behalf of the American Thoracic Society Assembly on Behavioral Science and Health Services Research
References
- 1.CDC. Asthma data, statistics, and surveillance: most recent asthma data. Atlanta, GA: CDC; 2019. https://www.cdc.gov/asthma/most_recent_data.htm [Google Scholar]
- 2. Akinbami LJ, Simon AE, Rossen LM. Changing trends in asthma prevalence among children. Pediatrics. 2016;137:1–7. doi: 10.1542/peds.2015-2354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Akinbami LJ, Moorman JE, Simon AE, Schoendorf KC. Trends in racial disparities for asthma outcomes among children 0 to 17 years, 2001-2010. J Allergy Clin Immunol. 2014;134:547–553, e5. doi: 10.1016/j.jaci.2014.05.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Urquhart A, Clarke P. US racial/ethnic disparities in childhood asthma emergent health care use: National Health Interview Survey, 2013–2015. J Asthma. 2019;57:510–520. doi: 10.1080/02770903.2019.1590588. [DOI] [PubMed] [Google Scholar]
- 5. Moonie SA, Sterling DA, Figgs L, Castro M. Asthma status and severity affects missed school days. J Sch Health. 2006;76:18–24. doi: 10.1111/j.1746-1561.2006.00062.x. [DOI] [PubMed] [Google Scholar]
- 6. Wang LY, Zhong Y, Wheeler L. Direct and indirect costs of asthma in school-age children. Prev Chronic Dis. 2005;2:A11. [PMC free article] [PubMed] [Google Scholar]
- 7. Kreger M, Sargent Cairoli K, Brindis CD. An underpinning of school inequities: asthma absences and lost revenue in California schools. J Sch Health. 2020;90:200–211. doi: 10.1111/josh.12869. [DOI] [PubMed] [Google Scholar]
- 8.Atlanta, GA: CDC; 2015. https://www.cdc.gov/asthma/asthma_stats/missing_days.htm [Google Scholar]
- 9.National Heart, Lung, and Blood Institute. Guidelines for the diagnosis and management of asthma: expert panel report 3. Washington, DC: U.S. Department of Health and Human Services; 2007. [Google Scholar]
- 10.National Heart, Lung, and Blood Institute. Managing asthma: a guide for schools. Washington, DC: U.S. Department of Health and Human Services; 2014. [Google Scholar]
- 11. American Thoracic Society. Guidelines for assessing and managing asthma risk at work, school, and recreation. Am J Respir Crit Care Med. 2004;169:873–881. doi: 10.1164/rccm.169.7.873. [DOI] [PubMed] [Google Scholar]
- 12.CDC. Atlanta, GA: CDC; 2019. https://www.cdc.gov/healthyschools/asthma/index.htm [Google Scholar]
- 13.American Lung Association. Chicago, IL: American Lung Association; 2020. https://www.lung.org/lung-health-diseases/lung-disease-lookup/asthma/asthma-education-advocacy/asthma-friendly-schools-initiative [Google Scholar]
- 14. Toups MM, Press VG, Volerman A. National analysis of state health policies on students’ right to self-carry and self-administer asthma inhalers at school. J Sch Health. 2018;88:776–784. doi: 10.1111/josh.12681. [DOI] [PubMed] [Google Scholar]
- 15. Gerald JK, Stroupe N, McClure LA, Wheeler L, Gerald LB. Availability of asthma quick relief medication in five Alabama school systems. Pediatr Allergy Immunol Pulmonol. 2012;25:11–16. doi: 10.1089/ped.2011.0118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Volerman A, Toups M, Hull A, Dennin M, Kim TY, Ignoffo S, et al. Assessing children’s readiness to carry and use quick-relief inhalers. J Allergy Clin Immunol Pract. 2019;7:1673–1675.e2. doi: 10.1016/j.jaip.2018.11.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Volerman A, Kim TY, Sridharan G, Toups M, Hull A, Ignoffo S, et al. A mixed-methods study examining inhaler carry and use among children at school. J Asthma. 2020;57:1071–1082. doi: 10.1080/02770903.2019.1640729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Flores G, Snowden-Bridon C, Torres S, Perez R, Walter T, Brotanek J, et al. Urban minority children with asthma: substantial morbidity, compromised quality and access to specialists, and the importance of poverty and specialty care. J Asthma. 2009;46:392–398. doi: 10.1080/02770900802712971. [DOI] [PubMed] [Google Scholar]
- 19. Byrne J, Schreiber ME, Nguyen TQ. Community hospital-school partnership to treat asthma episodes at school and improve management. J Sch Health. 2006;76:336–339. doi: 10.1111/j.1746-1561.2006.00124.x. [DOI] [PubMed] [Google Scholar]
- 20. Cabana MD, Ebel BE, Cooper-Patrick L, Powe NR, Rubin HR, Rand CS. Barriers pediatricians face when using asthma practice guidelines. Arch Pediatr Adolesc Med. 2000;154:685–693. doi: 10.1001/archpedi.154.7.685. [DOI] [PubMed] [Google Scholar]
- 21. Diette GB, Skinner EA, Markson LE, Algatt-Bergstrom P, Nguyen TTH, Clark RD, et al. Consistency of care with national guidelines for children with asthma in managed care. J Pediatr. 2001;138:59–64. doi: 10.1067/mpd.2001.109600. [DOI] [PubMed] [Google Scholar]
- 22. Pulcini J, DeSisto MC, McIntyre CL. An intervention to increase the use of asthma action plans in schools: a MASNRN study. J Sch Nurs. 2007;23:170–176. doi: 10.1177/10598405070230030801. [DOI] [PubMed] [Google Scholar]
- 23. Jones SE, Wheeler LS, Smith AM, McManus T. Adherence to National Asthma Education and Prevention Program’s “How Asthma-Friendly Is Your School?” recommendations. J Sch Nurs. 2009;25:382–394. doi: 10.1177/1059840509343292. [DOI] [PubMed] [Google Scholar]
- 24. Greiling AK, Boss LP, Wheeler LS. A preliminary investigation of asthma mortality in schools. J Sch Health. 2005;75:286–290. doi: 10.1111/j.1746-1561.2005.00039.x. [DOI] [PubMed] [Google Scholar]
- 25. Becker JM, Rogers J, Rossini G, Mirchandani H, D’Alonzo GE., Jr Asthma deaths during sports: report of a 7-year experience. J Allergy Clin Immunol. 2004;113:264–267. doi: 10.1016/j.jaci.2003.10.052. [DOI] [PubMed] [Google Scholar]
- 26. Shah S, Gibson PG, Wachinger S. Recognition and crisis management of asthma in schools. J Paediatr Child Health. 1994;30:312–315. doi: 10.1111/j.1440-1754.1994.tb00652.x. [DOI] [PubMed] [Google Scholar]
- 27. Allen K, Henselman K, Laird B, Quiñones A, Reutzel T. Potential life-threatening events in schools involving rescue inhalers, epinephrine autoinjectors, and glucagon delivery devices: reports from school nurses. J Sch Nurs. 2012;28:47–55. doi: 10.1177/1059840511420726. [DOI] [PubMed] [Google Scholar]
- 28. Gerald LB, Snyder A, Disney J, Gerald JK, Thomas A, Wilcox G, et al. Implementation and evaluation of a stock albuterol program for students with asthma. Ann Am Thorac Soc. 2016;13:295–296. doi: 10.1513/AnnalsATS.201510-683LE. [DOI] [PubMed] [Google Scholar]
- 29. Lowe AA, Gerald JK, Clemens CJ, Stern DA, Gerald LB. Managing respiratory emergencies at school: a county-wide stock inhaler program. J Allergy Clin Immunol. doi: 10.1016/j.jaci.2021.01.028. [DOI] [PubMed] [Google Scholar]
- 30. Gerald LB, Strother J, Burkholder B, Gerald JK. Translating research into health policy: stock albuterol Legislation. Ann Am Thorac Soc. 2018;15:413–416. doi: 10.1513/AnnalsATS.201708-639HP. [DOI] [PubMed] [Google Scholar]
- 31. O’Rourke A, Zimmerman A, Platt H, Pappalardo AA. Preventing asthma emergencies in schools. Pediatrics. 2020;145:e20191995. doi: 10.1542/peds.2019-1995. [DOI] [PubMed] [Google Scholar]
- 32.Fraley T, O’Rourke A, Weiler A, Zimmerman A. Chicago, IL: Respiratory Health Association and Legal Council for Health Justice; 2018. https://resphealth.org/wp-content/uploads/2018/04/RHA_LCHJ-Issue-Brief-Asthma-Rescue-Medication-in-Schools-FINAL.pdf [Google Scholar]
- 33.Respiratory Health Association; Legal Council for Health Justice. 2018. [Google Scholar]
- 34.Fifty-Fourth Legislature, 2019-2020 Phoenix, AZ: Arizona State Legislature; 2020https://www.azleg.gov/sunset_review.pdf. [Google Scholar]
- 35. Gerald JK, Wechsler ME, Martinez FD. Asthma medications should be available for over-the-counter use: pro. Ann Am Thorac Soc. 2014;11:969–974. doi: 10.1513/AnnalsATS.201404-139OI. [DOI] [PubMed] [Google Scholar]
- 36. Douglass JA, Goeman DP, McCarthy EA, Sawyer SM, Aroni RA, Stewart K, et al. Over-the-counter β2-agonist purchase versus script: a cross-sectional study. Respir Med. 2012;106:223–229. doi: 10.1016/j.rmed.2011.09.012. [DOI] [PubMed] [Google Scholar]
- 37. Ramsdell JW, Klinger NM, Ekholm BP, Colice GL. Safety of long-term treatment with HFA albuterol. Chest. 1999;115:945–951. doi: 10.1378/chest.115.4.945. [DOI] [PubMed] [Google Scholar]
- 38. Raphael G, Taveras H, Iverson H, O’Brien C, Miller D. Twelve- and 52-week safety of albuterol multidose dry powder inhaler in patients with persistent asthma. J Asthma. 2016;53:187–193. doi: 10.3109/02770903.2015.1070862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Papp EM, Gerald JK, Sadreameli SC, Gerald LB. Why every school should have a stock inhaler: one nurse’s experience. Am J Public Health. 2019;109:1528–1529. doi: 10.2105/AJPH.2019.305314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Lowe AA. Stock inhaler programs: a quick reference guide to implementation for schools. Tucson, AZ: University of Arizona; 2020
- 41.National Association of School Nurses Silver Spring, MD: National Association of School Nurses; 2020https://www.nasn.org/advocacy/professional-practice-documents/position-statements/ps-workload. [DOI] [PubMed] [Google Scholar]
- 42.U.S. Food and Drug Administration. Silver Spring, MD: U.S. Food and Drug Administration; 2020. https://www.fda.gov/safety/recalls-market-withdrawals-safety-alerts [Google Scholar]
- 43. Goodwin JL, Gerald LB, Johnson JLH, Gerald JK. Use of a disposable valved-holding chamber (spacer) in a school-based asthma trial. J Allergy Clin Immunol Pract. 2018;6:307–309. doi: 10.1016/j.jaip.2017.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Payares-Salamanca L, Contreras-Arrieta S, Florez-García V, Barrios-Sanjuanelo A, Stand-Niño I, Rodriguez-Martinez CE. Metered-dose inhalers versus nebulization for the delivery of albuterol for acute exacerbations of wheezing or asthma in children: a systematic review with meta-analysis. Pediatr Pulmonol. 2020;55:3268–3278. doi: 10.1002/ppul.25077. [DOI] [PubMed] [Google Scholar]
- 45.CDC. Atlanta, GA: CDC; 2021. https://www.cdc.gov/coronavirus/2019-ncov/community/schools-childcare/index.html [Google Scholar]
- 46.Banner University Medical Center Tucson; Pima County Health Department; Thayer Medical; Asthma and Airway Disease Research Center, The University of Arizona Health Sciences. Tucson, AZ: Pima County Health Department; 2019. [Google Scholar]