
Figure 1: Illustration of various advanced common bile duct cannulation techniques.
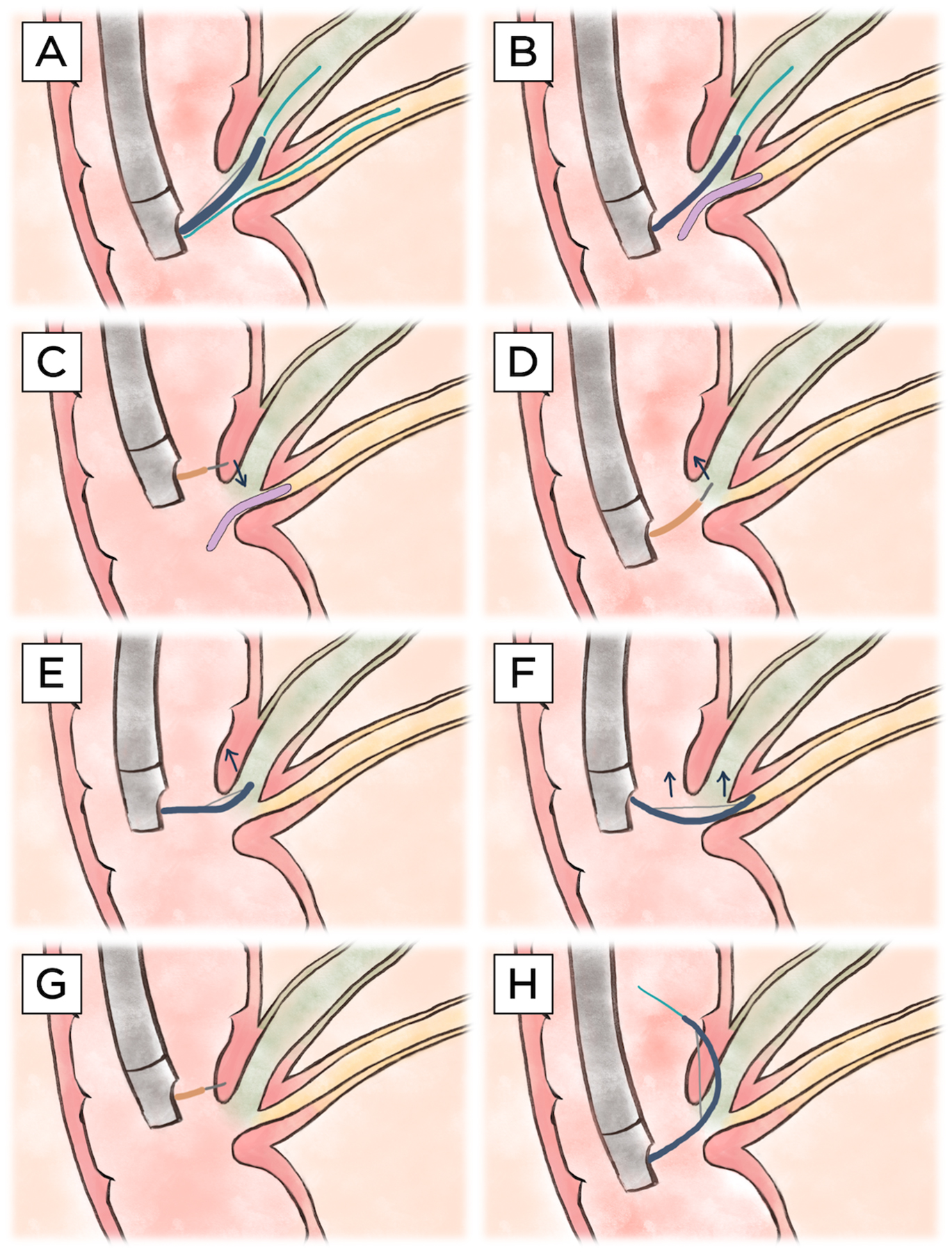
A) Double-guidewire technique. A guidewire (light blue) is first placed (often inadvertently) in the main pancreatic duct (yellow). This facilitates adjacent advancement of a second guidewire through a sphincterotome (blue) into the hepatopancreatic ampulla (via either a no-touch or touch technique) and thereafter into the common bile duct (green). B) Pancreatic stent-assisted technique. A pancreatic duct stent (purple) is first placed over a guidewire in the main pancreatic duct. Similar to the double-guidewire technique, this technique facilitates adjacent placement of a guidewire through a sphincterotome into the hepatopancreatic ampulla and onward into the common bile duct. C) Precut sphincterotomy over a pancreatic duct stent. A needle-knife catheter (orange) is used to cut inferiorly, starting suprapapillary in the (expected) location of the intraduodenal segment of the hepatopancreatic ampulla, towards the pancreatic duct stent. D) Precut papillotomy. A needle-knife is used to cut superiorly in a biliary (11–12 o’clock) orientation (i.e., vector), starting from the papillary orifice. E) Pull-type precut. A (semi-)seated sphincterotome is used to cut superiorly in a biliary orientation, starting from the papillary orifice. F) Transpancreatic precut sphincterotomy. A sphincterotome is inserted into the hepatopancreatic ampulla/distal pancreatic duct and, when repositioning into the distal bile duct is not feasible, used to cut superiorly, cutting through the septum in a biliary orientation. G) Precut supra-papillary fistulotomy. A needle-knife is used to incise directly into the intraduodenal segment of the distal bile duct/proximal hepatopancreatic ampulla, superior to the level of the papillary orifice. H) Intramural incision. After inadvertent creation of a false tract with a guidewire through the intraduodenal segment of the common bile duct, a sphincterotome is used to unroof the papilla to facilitate direct cannulation. Note: all illustrations show a major papilla with a conventional hepatopancreatic ampulla (i.e., a shared ductal orifice and normal common channel length); however, technique may vary in the case of variant (peri-) ampullary anatomy.