

Abstract
Background:
A large body of literature has reported positive effects of green space (GS) on various aspects of health and well-being, while no studies explore the role of GS in bone health.
Objectives:
The present study aimed to investigate the associations of GS with bone mineral density (BMD) change and incident fracture in a prospective cohort of elderly Hong Kong Chinese.
Methods:
Between 2001 and 2003, 3944 participants aged 65 years and older at baseline were recruited. GS (%) within 300-m and 500-m buffers were calculated for each participant based on the Normalized Difference Vegetation Index. BMD at whole body, lumbar spine, total hip, and femoral neck were assessed by dual energy X-ray absorptiometry at baseline and 3 follow-ups. Incident fracture cases were ascertained from the electronic database of Hospital Authority of Hong Kong. Linear mixed-effects models and Cox proportional hazards models were used to investigate the associations of GS with changes in BMD and incident fracture, respectively.
Results:
Greater GS within 300-m and 500-m buffers were associated with a slower increase in lumbar spine BMD over 14 years. After adjustment for potential confounders, β and 95% confidence intervals (CIs) of change in BMD across Q2-Q4 (quartiles of GS measured in a 300-m, compared with Q1) were −6.42 (−12.3, −0.59), −7.78 (−13.6, −1.97), and −7.83 (−13.7, −2.00) mg/cm3, respectively. GS was also positively associated with non-spinal fracture and major osteoporotic fracture incidence risks. Multivariable-adjusted hazard ratios (95%CIs) were 1.40 (1.09, 1.79; P-trend=0.036) for non-spinal fracture and 1.53 (1.13, 2.07; P-trend=0.010) for major osteoporotic fracture (Q4 compared with Q1 of GS measured in a 300-m buffer). Positive GS-fracture associations were also found for GS within a 500-m buffer.
Conclusions:
We found that those who lived near higher GS levels had a slower increase in lumbar spine BMD and had higher incident fracture risk.
Keywords: green space, bone mineral density, fracture, dual energy X-ray absorptiometry, cohort study
1. Introduction
Osteoporosis has been a global health problem worldwide, with an estimated 200 million people being affected globally (Vijayakumar et al., 2016) and 60.2 million people aged 50 years and older have been estimated to have osteoporosis in China (Zeng et al., 2019). Osteoporosis is one of the key risk factors of fracture, which is positively associated with mortality risk (Lee et al., 2021).
There has been an ongoing interest in the role of environmental factors, such as air pollution, in the development of osteoporosis in the past decade. Air pollution (e.g., particulate matter 2.5 and 10) may cause systemic inflammation, oxidative damage, and vitamin D deficiency, which can be linked to bone mineral density (BMD) loss, osteoporosis development (Bind et al., 2012; Feizabad et al., 2017; Prada et al., 2020), and life expectancy loss (Qi et al., 2020; Tian et al., 2020; Yang et al., 2020). Epidemiological studies have also highlighted that exposure to air pollution is positively associated with higher osteoporosis risk and lower BMD (Liu et al., 2021; Mazzucchelli et al., 2018; Oh and Song 2020; Prada et al., 2017; Qiao et al., 2020; Ranzani et al., 2020; Sung et al., 2020). Therefore, improvement of air quality may be an important way to prevent osteoporosis.
Green space (GS), which is one of the most studied built environment features, has been well linked to human health. A large body of literature has reported the positive health effect of GS. For example, higher GS levels are associated with better physical functioning, lower body mass index (BMI), lower cardiovascular disease risk, and lower mortality risk (de Keijzer et al., 2019; Fuertes and Jarvis 2021; Ji et al., 2019; Klompmaker et al., 2018; Teixeira et al., 2021; Yuan et al., 2020). There is growing evidence that GS can reduce air pollution levels, which may be one of the mechanisms underlying the health benefits of GS (Dzhambov et al., 2020; Markevych et al., 2017). In addition to mediating through air pollution, multiple pathways are suggested to explain the associations of GS with well-being and health, of which physical activity (PA) is the most common pathway for linking GS to health since the health benefits of PA are well documented (Dzhambov et al., 2020; Markevych et al., 2017). It is also well documented that PA and BMI are key determinants of BMD. Besides, we mentioned above that air pollution is associated with BMD loss. Thus, we hypothesized that GS may play a role in the development of bone health.
However, to the best of our knowledge, there is no study investigating the role of GS in bone health. Therefore, we aimed to investigate the associations of GS with BMD change and incident fracture in a prospective cohort of elderly Hong Kong Chinese citizens in Hong Kong.
2. Materials and methods
2.1. Study design and population
Participants in the current study were from a prospective cohort (Mr. OS and Ms. OS Hong Kong Study), the first large-scale cohort study designed to investigate the determinants of bone health in elderly Chinese men and women (Kwok et al., 2017; Lin et al., 2020; Su et al., 2017). A total of 4000 elderly Chinese men and women (2000 men and 2000 women, respectively) aged 65 years or above were recruited from Hong Kong communities between August 2001 and December 2003. The participants were prospectively followed until November 2015-September 2017, with 4 rounds of follow-up (Figure 1). Those who were unable to walk independently and provide written informed consent were excluded. The cohort study was approved by the Clinical Research Ethics Committee of the Chinese University of Hong Kong, and all participants provided written informed consent.
Figure 1. Flowchart of study participants over study period.
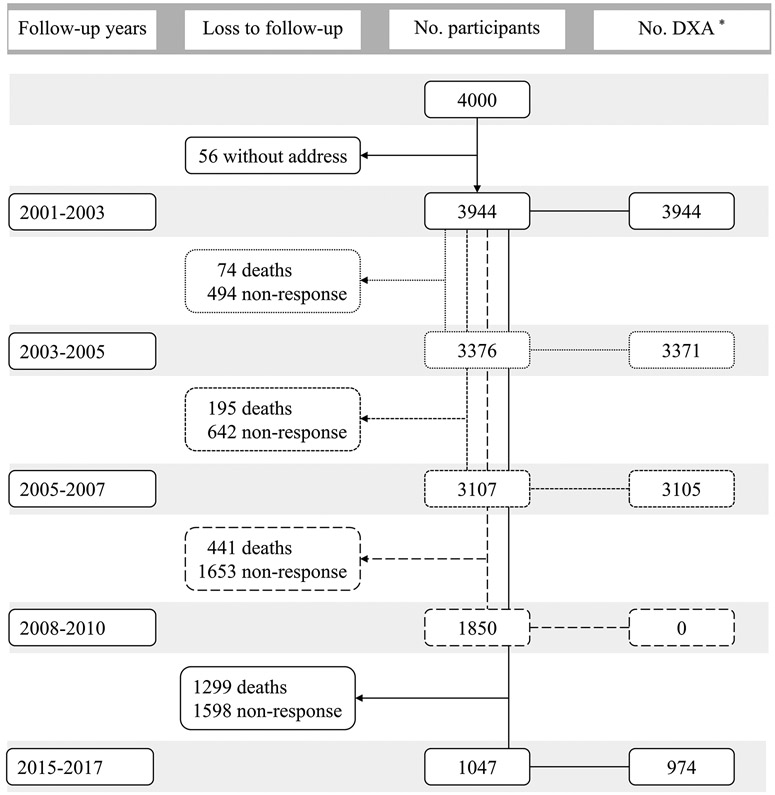
* Number of participants whose bone mineral density was assessed by dual energy X-ray absorptiometry (DXA).
2.2. Measurement of green space
Detailed information on the measurement of GS was published elsewhere (Lin et al., 2021; Wang et al., 2017). In brief, the Normalized Difference Vegetation Index (NDVI), which was calculated from IKONOS multispectral images was used to represent GS (Nichol et al., 2006). NDVI measures the amount of vegetation over a unit area and ranges from −1 (water) to +1 (completely vegetated areas). A vegetation map was created using ArcGIS 10.3 software (ESRI Inc, Redlands, CA, USA), with a spatial resolution of 15*15 m for each pixel. A pixel was identified as GS if the value was ≥ 0.1. We used a 300-m and a 500-m Euclidean buffer (about 5-min and 10-min walking distance for our participants, respectively (Yu et al., 2014)) around participants’ addresses to calculate the GS that the participants were exposed to. The percentage of GS within the buffer zone of the participants’ address was calculated by counting the number of pixels identified as GS. Figure S1 shows the geographical distribution of the participants’ baseline addresses by quartiles of GS.
2.3. Assessment of BMD and fracture incidence
BMD at Whole body and regional areas (lumbar spine[L1-L4], total hip, and femoral neck) were measured by dual-energy X-ray absorptiometry (Hologic QDR 4500 W densitometer, Hologic, Waltham, MA, USA) at each survey, except the third follow-up (2008-2010, Figure 1). The coefficients of variation were 1.0%, 0.9%, 0.7%, and 1.3% for whole body, lumbar spine, total hip, and femoral neck, respectively, and calibration was performed daily on a lumbar spine phantom (Kwok et al., 2012; Tang et al., 2010).
Participants were followed up for fracture incidence at each survey when came to the research center and followed up via telephone calls every 4 months in the first 4 years after baseline visit. We also searched the electronic database of Hospital Authority of Hong Kong, which includes all visits to the Accident and Emergency Department and outpatient clinics in any publicly funded hospitals in Hong Kong for up to 10 years or more. Data updated on 31 October 2013 (men) and 31 May 2012 (women) were used in the present analysis. The fracture sites and degree of trauma of the incident fracture were also recorded. Non-traumatic incident fractures were included in the present analysis, while spinal fractures were excluded. Osteoporotic fractures were defined as fractures occurring from a fall from a standing height or less, without major trauma. Non-traumatic major osteoporotic fractures (hip, spine, forearm, and shoulder) were also included.
2.4. The questionnaire and physical measurements
A standardized and structured questionnaire was conducted by trained investigators. Information on age, sex, marital status, education level, socioeconomic status [SES] (Adler et al., 2000)), alcohol drinking, smoking, calcium supplement, PA (Washburn et al., 1993)), history of chronic diseases and medications, previous history of fracture, and family history of fracture were collected. Number of chronic diseases was calculated through 12 common chronic diseases or symptoms (e.g., hypertension and cardiovascular disease). Anthropometric measurements were also conducted, and BMI was calculated as weight (kg)/height (m)2. Data collection has been described in detail in our previous studies, such as the items to measure each variable (Lin et al., 2021; Lin et al., 2020).
2.5. Statistical analyses
2.5.1. Descriptive analyses
Characteristics of participants and BMD over the study period were described. Baseline characteristics of study population by quartiles (Q) of GS and difference in population characteristics between participants with and without follow-up information on BMD were examined by ANOVA (continuous variables) or chi-squared test (categorical variables).
2.5.2. Associations of GS with annual change in BMD
Participants without information on addresses (n=56) or BMD were excluded from this analysis. A total of 3944 participants with 11394 observations were included (Figure 1), and the mean follow-up time was 6.4 years. Linear mixed-effects models were used to estimate β and 95% confidence intervals (CIs) of change in BMD across Q2 to Q4 of GS compared with Q1. The fixed effect included quartiles of GS, age, and their interaction term, and the person as a random effect (random intercept). Age was used as a timescale. Age was centered at mean age at baseline (72.5 years) and divided by 14 to give 14 years change. The interaction term of GS with age could be interpreted as the impact of GS on 14 years change in BMD. We constructed 2 statistical models: model 1 included time-varying covariates (age, marital status, alcohol drinking, smoking, BMI, PA, calcium supplement, and number of chronic diseases) and time-constant covariates (i.e., baseline characteristics, including sex, education level, SES, and any incident fracture). Model 2 further adjusted for baseline BMD (whole body, lumbar spine, total hip, and femoral neck, respectively).
2.5.3. Associations of GS with incident fracture
We included 3944 participants with a valid address at baseline and used the Cox proportional hazards models to estimate hazard ratios (HRs) and 95%CIs across Q2 to Q4 compared with Q1 for incident fracture. Survival time was calculated from the date of the first survey until the date of the first fracture incidence or the latest fracture data updated (2012-2013), whichever came first. We also constructed 2 statistical models: model 1 adjusted for baseline age, sex, marital status, education level, SES, alcohol drinking, smoking, BMI, PA, calcium supplement, number of chronic diseases, previous history of fracture, and family history of fracture; model 2 further adjusted for baseline BMD at whole body. P-trends were calculated from the associations of per 1 standard deviation increase in GS with incident fracture.
Restricted cubic spline models with 3 knots (at 10th, 50th, and 90th) were used to explore the shape of the associations of GS with incident fracture in the Cox proportional hazards models, adjusting for the covariates as in the above model 2. P-values for nonlinearity were calculated using a Wald test.
2.5.4. Sensitivity analyses
Sensitivity analyses were performed based on the final model (i.e., model 2) to test the robustness of our findings. We repeated the linear mixed-effects models and Cox proportional hazards models after excluding participants who reported moving from the baseline address during follow-up.
All analyses were conducted by R version 4.0.3 and RStudio version 1.3. A two-tailed P-value <0.05 was considered statistically significant.
3. Results
3.1. Descriptive analyses
The mean BMD at whole body and lumbar spine tended to increase over the study period, while BMD at total hip and femoral neck tended to decrease (Table S1). Table 1 shows that participants with higher GS (300-m buffer) tended to be female, less educated, and had lower BMD at whole body, total hip, and femoral neck. Baseline characteristics of participants by GS in a 500-m buffer are shown in Table S2. Characteristics between participants with and without follow-up information on BMD are shown in Table S3. Participants lost to follow-up tended to be older, widowed/single, less educated, smoker, consumed less alcohol and calcium supplement, had a higher proportion of participants with chronic diseases, had lower PA levels, and had lower BMD.
Table 1.
Baseline characteristics of participants by quartiles (Q) of green space (300-m buffer)
| Characteristics | Q1 (n=998) | Q2 (n=983) | Q3 (n=980) | Q4 (n=983) |
P- value a |
|---|---|---|---|---|---|
| Mean (standard deviation) or number (%) | |||||
| Green space, %, median (range) | 1.59 (0.00-4.54) | 7.96 (4.54-13.21) | 21.0 (13.21-34.14) | 49.3 (34.14-100) | NA |
| Age, years | 72.54 (5.20) | 72.27 (5.14) | 72.56 (5.22) | 72.53 (5.20) | 0.566 |
| Sex, female, N (%) | 461 (46.2) | 484 (49.2) | 514 (52.4) | 513 (52.2) | 0.017 |
| Marital status, N (%) | 0.776 | ||||
| Married | 727 (72.8) | 702 (71.5) | 684 (69.8) | 682 (69.5) | |
| Widowed | 226 (22.6) | 240 (24.4) | 255 (26.1) | 250 (25.4) | |
| Separated or divorced | 22 (2.3) | 19 (1.9) | 20 (2.0) | 27 (2.7) | |
| Single (never married) | 23 (2.3) | 22 (2.2) | 21 (2.1) | 24 (2.4) | |
| Education level, N (%) | <0.001 | ||||
| No education | 182 (18.2) | 188 (19.1) | 249 (25.4) | 224 (22.8) | |
| Primary school or below | 509 (51.0) | 476 (48.4) | 468 (47.8) | 524 (53.3) | |
| Secondary school or above | 307 (30.8) | 319 (32.5) | 263 (26.8) | 235 (23.9) | |
| Socioeconomic status, N (%) | 0.215 | ||||
| Low (1-3) | 268 (26.9) | 307 (31.3) | 282 (28.8) | 310 (31.5) | |
| Middle (4-6) | 598 (59.9) | 549 (55.8) | 558 (56.9) | 553 (56.3) | |
| High (7-10) | 132 (13.2) | 127 (12.9) | 140 (14.3) | 120 (12.2) | |
| Alcohol drinking, N (%) | 130 (13.0) | 141 (14.3) | 117 (11.9) | 127 (12.9) | 0.470 |
| Smoking, N (%) | 70 (7.0) | 67 (6.8) | 63 (6.4) | 73 (7.4) | 0.852 |
| Calcium supplement, N (%) | 145 (14.5) | 147 (15.0) | 134 (13.7) | 119 (12.1) | 0.269 |
| No. chronic diseases, N (%) | 0.061 | ||||
| 0 | 179 (17.9) | 178 (18.1) | 146 (14.9) | 145 (14.8) | |
| 1 or 2 | 540 (54.1) | 539 (54.8) | 530 (54.1) | 573 (58.2) | |
| ≥ 3 | 279 (28.0) | 266 (27.1) | 304 (31.0) | 265 (27.0) | |
| Previous history of fracture, N (%) | 173 (17.3) | 167 (17.0) | 159 (16.2) | 178 (18.1) | 0.737 |
| Family history of fracture, N (%) | 48 (4.8) | 58 (5.9) | 37 (3.8) | 54 (5.5) | 0.148 |
| Body mass index, kg/m2 | 23.79 (3.29) | 23.75 (3.24) | 23.72 (3.26) | 23.49 (3.40) | 0.161 |
| PASE score | 90.45 (42.93) | 92.02 (42.03) | 89.81 (42.76) | 92.46 (43.63) | 0.467 |
| Bone mineral density, g/cm3 | |||||
| Whole body | 0.99 (0.12) | 0.99 (0.13) | 0.98 (0.13) | 0.98 (0.12) | 0.015 |
| Lumbar spine | 0.86 (0.19) | 0.86 (0.20) | 0.85 (0.19) | 0.84 (0.19) | 0.138 |
| Total hip | 0.80 (0.14) | 0.79 (0.14) | 0.78 (0.15) | 0.77 (0.15) | <0.001 |
| Femoral neck | 0.64 (0.12) | 0.64 (0.12) | 0.63 (0.11) | 0.63 (0.12) | 0.004 |
Abbreviations: PASE, Physical Activity Scale for the Elderly.
P-value was estimated by ANOVA (continuous variables) or chi-squared test (categorical variables).
3.2. Associations of GS with annual change in BMD
There were significant associations between GS measured in a 300-m buffer and annual changes in BMD at whole body, lumbar spine, total hip, and femoral neck over 14 years in model 1, adjusting for socio-demographic characteristics, lifestyle factors, and history of chronic diseases (Table 2 and Figure 2). However, after further adjustment for baseline BMD in model 2, no associations of GS with changes in BMD at total hip and femoral neck were observed. Greater GS was associated with a slower decrease in whole body BMD in model 2 and β (95%CIs) were 5.41 (0.50, 10.3) mg/cm3 for Q2, 2.18 (−2.74, 7.09) mg/cm3 for Q3, and 5.58 (0.66, 10.5) for Q4 compared with Q1. In contrast, greater GS was associated with a slower increase in lumbar spine BMD in model 2 and β (95%CIs) across Q2-Q4 were −6.42 (−12.3, −0.59), −7.78 (−13.6, −1.97), and −7.83 (−13.7, −2.00) mg/cm3, respectively. Table 2 also shows the associations of GS measured in a 500-m buffer with changes in BMD. We observed that higher GS was only significantly associated with a slower increase in lumbar spine BMD in model 2. There was no substantial difference in sensitivity analyses (Table S4).
Table 2.
Associations of green space with annual change in bone mineral density (mg/cm3) over 14 years (case=3944; observation=11394) a
| Model | Quartiles (Q) of green space | ||||
|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | ||
| 300-m buffer | |||||
| Whole body | Model 1 b | Reference | 8.83 (1.72, 15.9) * | 2.31 (−4.85, 9.48) | 5.35 (−1.74, 12.4) |
| Model 2 c | Reference | 5.41 (0.50, 10.3) * | 2.18 (−2.74, 7.09) | 5.58 (0.66, 10.5) * | |
| Lumbar spine | Model 1 b | Reference | −15.9 (−24.5, −7.21) *** | −17.6 (−26.3, −8.90) *** | −18.7 (−27.4, −10.1) *** |
| Model 2 c | Reference | −6.42 (−12.3, −0.59) * | −7.78 (−13.6, −1.97) ** | −7.83 (−13.7, −2.00) ** | |
| Total hip | Model 1 b | Reference | 2.26 (−2.60, 7.12) | −6.79 (−11.7, −1.89) ** | −1.09 (−5.94, 3.76) |
| Model 2 c | Reference | 1.45 (−2.23, 5.13) | −3.06 (−6.74, 0.62) | 0.70 (−2.98, 4.39) | |
| Femoral neck | Model 1 b | Reference | 3.17 (−2.22, 8.57) | −6.00 (−11.4, −0.57) * | −3.02 (−8.41, 2.36) |
| Model 2 c | Reference | 1.54 (−2.29, 5.37) | −1.56 (−5.38, 2.26) | −1.87 (−5.70, 1.96) | |
| 500-m buffer | |||||
| Whole body | Model 1 b | Reference | −1.38 (−8.55, 5.79) | 0.05 (−7.00, 7.09) | 0.27 (−6.89, 7.44) |
| Model 2 c | Reference | −0.95 (−5.90, 4.01) | 0.82 (−4.04, 5.68) | 2.88 (−2.08, 7.84) | |
| Lumbar spine | Model 1 b | Reference | −13.6 (−22.3, −4.90) ** | −20.6 (−29.2, −12.1) *** | −21.1 (−29.8, −12.4) *** |
| Model 2 c | Reference | −4.00 (−9.89, 1.88) | −7.30 (−13.1, −1.54) * | −9.09 (−15.0, −3.21) ** | |
| Total hip | Model 1 b | Reference | −5.30 (−10.2, −0.41) * | −6.38 (−11.2, −1.57) ** | −6.25 (−11.2, −1.36) * |
| Model 2 c | Reference | −0.13 (−3.84, 3.58) | −2.01 (−5.65, 1.63) | −1.20 (−4.91, 2.51) | |
| Femoral neck | Model 1 b | Reference | −3.48 (−8.92, 1.95) | −4.43 (−9.77, 0.92) | −6.98 (−12.4, −1.55) * |
| Model 2 c | Reference | 0.40 (−3.45, 4.25) | −1.86 (−5.64, 1.92) | −3.06 (−6.91, 0.80) | |
Linear mixed-effects models were used to estimate β (95% confidence interval) of change in bone mineral density across Q2 to Q4 compared with Q1.
Model 1: included age, green space (quartiles), and their interaction term, and adjusted for sex, marital status, education level, socioeconomic status, alcohol drinking, smoking, body mass index, physical activity, calcium supplement, number of chronic diseases, and any incident fracture.
Model 2: model 1 plus baseline bone mineral density (whole body, lumbar spine, total hip, and femoral neck, respectively).
P-value<0.05
P-value <0.01
P-value <0.001
Figure 2. Trajectories of bone mineral density over age by Quartiles (Q) of green space (300-m buffer).

Trajectories derived from linear mixed-effects models, including age, green space (quartiles), and their interaction term in the models, and adjusted for sex, marital status, education level, socioeconomic status, alcohol drinking, smoking, body mass index, physical activity, calcium supplement, number of chronic diseases, any incident fracture, and baseline bone mineral density (whole body, lumbar spine, total hip, and femoral neck, respectively). In comparison with Q1, Q4 had a slower decrease in whole body bone mineral density (Panel a), while a slower increase in lumbar spine bone mineral density (Panel b).
3.3. Associations of GS with incident fracture
During 36735 person-years of follow-up (mean follow-up of 9.3 years), 479 cases of incident non-spinal fracture and 340 cases of incident major osteoporotic fracture were identified. Detailed information on incident fracture has been reported previously (Kwok et al., 2017; Su et al., 2017). GS was positively associated with non-spinal fracture and major osteoporotic fracture incidence risks in both model 1 and model 2 (Table 3). In model 2, multivariable-adjusted HRs (95%CIs) were 1.40 (1.09, 1.79; P-trend=0.036) for non-spinal fracture and 1.53 (1.13, 2.07; P-trend=0.010) for major osteoporotic fracture (Q4 compared with Q1, GS measured in a 300-m buffer). The associations of GS measured in a 500-m buffer with incident fracture did not have a substantial difference with the above risk estimates. Table S5 also shows robust findings from sensitivity analyses.
Table 3.
Associations of green space with incident fracture in the Mr. OS and Ms. OS Study (N=3944) a
| Model | Quartiles (Q) of green space | P-trend | ||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | |||
| 300-m buffer | ||||||
| Non-spinal | No. participants | 998 | 983 | 977 | 986 | |
| Case/person-year | 108/9395 | 109/9091 | 111/9090 | 151/9159 | ||
| Model 1 b | 1.00 (ref) | 1.04 (0.80, 1.36) | 1.04 (0.80, 1.36) | 1.43 (1.11, 1.83) | 0.003 | |
| Model 2 c | 1.00 (ref) | 1.02 (0.79, 1.34) | 1.03 (0.79, 1.34) | 1.40 (1.09, 1.79) | 0.036 | |
| Major osteoporotic | No. participants | 998 | 983 | 977 | 986 | |
| Case/person-year | 70/9395 | 81/9091 | 80/9090 | 109/9159 | ||
| Model 1 b | 1.00 (ref) | 1.22 (0.88, 1.68) | 1.13 (0.82, 1.56) | 1.56 (1.15, 2.11) | 0.008 | |
| Model 2 c | 1.00 (ref) | 1.19 (0.86, 1.63) | 1.10 (0.80, 1.52) | 1.53 (1.13, 2.07) | 0.010 | |
| 500-m buffer | ||||||
| Non-spinal | No. participants | 987 | 986 | 991 | 980 | |
| Case/person-year | 102/9311 | 107/9082 | 118/9234 | 152/9107 | ||
| Model 1 b | 1.00 (ref) | 1.03 (0.78, 1.35) | 1.14 (0.88, 1.49) | 1.48 (1.15, 1.90) | 0.001 | |
| Model 2 c | 1.00 (ref) | 1.03 (0.78, 1.35) | 1.13 (0.87, 1.48) | 1.45 (1.13, 1.87) | 0.001 | |
| Major osteoporotic | No. participants | 987 | 986 | 991 | 980 | |
| Case/person-year | 70/9311 | 82/9082 | 85/9234 | 103/9107 | ||
| Model 1 b | 1.00 (ref) | 1.14 (0.83, 1.57) | 1.16 (0.85, 1.60) | 1.41 (1.04, 1.92) | 0.020 | |
| Model 2 c | 1.00 (ref) | 1.14 (0.83, 1.57) | 1.15 (0.84, 1.58) | 1.39 (1.02, 1.88) | 0.024 | |
The Cox proportional hazards models were used to estimate hazard ratios and 95% confidence intervals across Q2 to Q4 compared with Q1. P-trends were calculated from the associations of per 1 standard deviation increase in green space with incident fracture.
Model 1: adjusted for baseline age, sex, marital status, education level, socioeconomic status, alcohol drinking, smoking, body mass index, physical activity, calcium supplement, number of chronic diseases, previous history of fracture, and family history of fracture.
Model 2: model 1 plus baseline whole body bone mineral density.
We did not find evidence of nonlinearity in restricted cubic spline models (P-nonlinear >0.05), and the shapes of the associations of GS levels with incident non-spinal fracture are presented in Figure 3. Linear positive associations between GS and incident non-spinal fracture were noted in the above model 2 with per standard deviation HR 1.14 (95%CI 1.04, 1.24) for a 300-m buffer and 1.16 (1.06, 1.26) for a 500-m buffer.
Figure 3. Shapes of the associations of green space with incident non-spinal fracture.
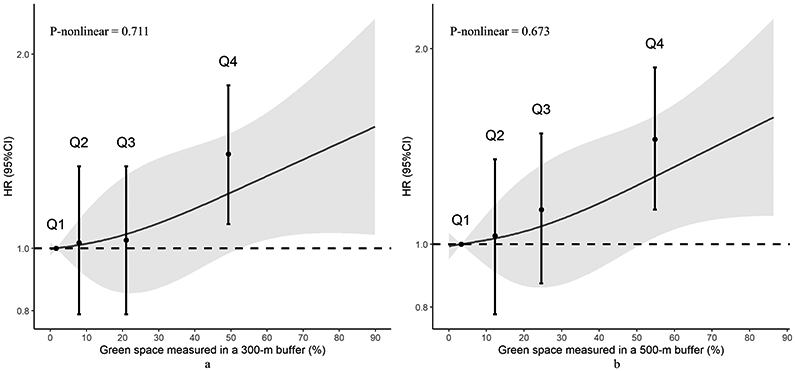
Restricted cubic spline models were used to estimate the associations of green space with incident non-spinal fracture in the Cox proportional hazards models, adjusted for baseline age, sex, marital status, education level, socioeconomic status, alcohol drinking, smoking, body mass index, physical activity, calcium supplement, number of chronic diseases, previous history of fracture, family history of fracture, and whole body bone mineral density. None of the associations showed significant nonlinearity (P-nonlinearity >0.05). In addition, to make the dose-response association comparable with the quartile (Q) results, we also plotted the hazard ratio (HR) and 95% confidence interval (95% CI) of incident fracture across Q2 to Q4 of green space (compared with Q1, location of each plot corresponds to the median levels within each quartile).
4. Discussion
We investigated the associations of GS with 14 years changes in BMD and incident fracture in a prospective cohort. We found that exposure to higher GS level was associated with a slower increase in lumbar spine BMD, but not associated with changes in BMD at total hip and femoral neck. No convincing association between higher GS and a slower decrease in whole body BMD was also observed (significant association was found for GS measured in a 300-m buffer, but not a 500-m buffer). We also found that GS was positively associated with risk of fracture incidence and robust findings were found for both 300-m and 500-m buffers.
To the best of our knowledge, this is the first study investigating the associations of GS with BMD and incident fracture. However, we failed to observe a protective effect of GS on bone health, which was against our hypothesis. Our findings were also inconsistent with previous findings that GS benefits various aspects of well-being and health, such as obesity (Huang et al., 2020; Luo et al., 2020) and mortality (Ji et al., 2020; Rojas-Rueda et al., 2019). We attempted to explain our findings by hypothesizing that the associations between GS and bone health may be mediated by PA, but it may be that participants living near higher GS levels were more likely to be less physical active. Two cross-sectional studies did report inverse associations of GS with walking and cycling (Maas et al., 2008; van Heeswijck et al., 2015).
The present study was conducted in older adults who resided in an ultra-high density city, Hong Kong, with most of its 7 million population living in medium or high density areas. Hong Kong is a highly compact city, which is characterized by high residential density with mixed land uses, and only 24.9% of land resources in Hong Kong are total urban or built-up land (HKPD 2019). Although the percentage of GS in Hong Kong is 65.4%, most of them are woodland (24.8%) and shrubland (23.8%) located in rural areas, which are not accessible to urban residents (HKPD 2019; Yuen et al., 2019). Some specific types of GS may not be valuable resources for PA. Previous studies indicated that the association between different types of GS and PA may be different (Coombes et al., 2010; Klompmaker et al., 2018; Lee and Maheswaran 2011; Miralles-Guasch et al., 2019). For instance, a cross-sectional study found that participants who lived near the type of GS identified as Formal parks (those with an organized layout and structured path network, and generally well maintained) had higher PA levels, while for other types of GS (e.g., natural GS and sports GS), different types of GS were associated with PA in different directions (Coombes et al., 2010). In our study, the GS that participants in the highest GS levels group (Q4) exposed to may be the type of GS that provides few opportunities to engage in PA. For instance, natural woodland, which has no recreational facilities, human-made pavement, and vacant lots for PA, is less likely to encourage the elderly to engage in PA. Besides, much of Hong Kong's land consists of natural and undeveloped terrain, which is from hilly to mountainous, with steep slopes and very little flat land (Morton and Harper 1995). Thus, such hilly or sloping GS may also have an adverse impact on the PA of the elderly living in Hong Kong. In addition, part of GS may be private GS, which is not accessible to the public. The above evidence may partially explain our findings that participants with the highest GS levels (Q4) did not have a slower decline in BMD and lower fracture risk compared with participants with the lowest GS levels (Q1). However, we did not have data on the types of GS, and therefore, we were unable to investigate how different types of GS may be associated with BMD changes and incident fracture risk.
On the other hand, there are potentially adverse influences of GS (Evensen et al., 2021; Fan et al., 2020; Herzog and Kutzli 2002; Jansson et al., 2013). GS has been found to be associated with increased feelings of unsafety and fear of crime, because GS such as woodland may be perceived as a dangerous hiding place for crime activities (Evensen et al., 2021; Herzog and Kutzli 2002; Jansson et al., 2013). Such fear of crime may discourage people to engage in PA in GS and previous studies have reported that lower perceived safety of GS was associated with lower PA levels (Evenson et al., 2012; Jackson and Stafford 2009; Rees-Punia et al., 2018).
Besides, there are also potential negative effects related to engaging in PA in GS, such as falls, which is one of the key determinants of fracture (Nilsson et al., 2016; Winstead et al., 2021). Engaging in PA may increase the older adults’ chance of falling, and our prior study found that highly active older adults had higher fall rates compared with moderately active older adults (Lu et al., 2020). Another potential explanation for the higher risk of incident fracture among participants with higher GS is that these participants are more likely to live near rural areas, since most GS in Hong Kong are located in rural areas. The roads are less safe in rural areas (e.g., poor lighting and bumpiness), which may also increase the chance of falling.
Differences in socio-economic characteristics (e.g., SES and education level) between participants living near lower and higher levels of GS may also help to explain our findings. In Hong Kong, the government provides public rental housing estates to socioeconomically disadvantaged groups at affordable prices. In 2016, 30.4% of domestic households in Hong Kong were living in public rental housing estates, and 53% were in private permanent housing (Census and Statistics Department 2017). The public housing estates are built with greener designs to create a green and healthy living environment for public housing residents, while for the private housing, all the shared spaces and facilities are paid by the owners (Chan et al., 2008). Thus, residents with low-SES are common living near higher GS than residents with high-SES. Our results also show that participants with higher GS tended to be less educated and low-SES (Table 1). Previous studies have indicated that low-SES and low education level are associated with poor nutritional intake and PA that leads to lower BMD (Brennan et al., 2011; Du et al., 2017).
Our study has several strengths. Firstly, we used objective measurements of GS and BMD, and BMD was measured for 4 times over 14 years. Secondly, to the best of our knowledge, our study is the first study investigating the associations of GS with BMD and incident fracture, and based on a large sample prospective cohort.
Several limitations should be considered. Firstly, we only measured GS at baseline, while the GS around participants’ addresses may change during follow-up or participants may move to the new addresses. These may cause potential exposure misclassification. However, the results of sensitivity analyses did not change materially after excluding participants who reported moving from the baseline address during follow-up. Secondly, we did not have data on the specific types of GS that participants were exposed to, which did not allow us to estimate how different types of GS may affect BMD change and incident fracture, nor did we have information on participants’ use of GS. Besides, we had no information on the quality, accessibility, and safety of GS. Thus, we were unable to explore the potential mechanisms underlying our findings. Thirdly, there were differences in population characteristics between participants with and without follow-up information on BMD, so participants lost to follow-up may cause selection bias. Finally, our study was conducted in older adults (aged 65 years and older) who resided in an ultra-high density city, Hong Kong, and therefore, the generalization of our findings should be cautious.
5. Conclusions
In conclusion, in this prospective cohort of elderly Hong Kong Chinese who resided in an ultra-high density city, we found that people living near higher GS levels had a slower increase in lumbar spine BMD and had higher incident fracture risk compared with people living near lower GS levels. However, we were unable to explore the underlying mechanisms due to an absence of data on the specific types, qualities, and participants’ use of GS. The relationships between GS and health outcomes are complex and represent a component of the overall impact of urban design and neighborhood factors. We were unable to take these into account, and future studies employing a composite model may be able to address these questions in greater detail. More studies are warranted to replicate our findings.
Supplementary Material
Table S1. Characteristics of participants and bone mineral density over the study period
Table S2. Baseline characteristics of participants by quartiles (Q) of green space (500-m buffer)
Table S3. Baseline characteristics for participants with and without follow-up information on bone mineral density
Table S4. Sensitivity analysis for associations of green space with annual change in bone mineral density (mg/cm3) over 14 years
Table S5. Sensitivity analysis for associations of green space with incident fracture in the Mr. OS and Ms. OS Study.
Figure S1. Geographical distribution of the participants’ baseline addresses by quartiles (Q) of green space.
Acknowledgments
We thank all the participants and staff who contributed to the present study. We thank the generous donation of Ms. Therese Pei Fong Chow. J.-S.L. would like to thank the China Scholarship Council (CSC) for the financial support (No. 202008440343).
Funding
K.K.-L.K. was funded by the Vice-Chancellor’s One-off Discretionary Fund of the Chinese University of Hong Kong (No.: 4930785) and the Direct Grant for Research 2017/18 of the Faculty of Social Science, the Chinese University of Hong Kong (No.: 4052187). The study was also supported by the National Institutes of Health R01 Grant AR049439–01A1 and the Chinese University of Hong Kong Research Grants Council Earmarked Grant CUHK4101/02M. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Abbreviations:
- BMD
Bone mineral density
- BMI
Body mass index
- CIs
Confidence intervals
- GS
Green space
- HRs
Hazard ratios
- NDVI
Normalized Difference Vegetation Index
- PA
Physical activity
- PASE
Physical Activity Scale for the Elderly
- Q
Quartiles
- SES
Socioeconomic status
Footnotes
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ethics statement
The study was approved by the Clinical Research Ethics Committee in the Chinese University of Hong Kong, and all participants provided written informed consent.
References
- Adler NE; Epel ES; Castellazzo G; Ickovics JR Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy white women. Health Psychol. 2000;19:586–592 [DOI] [PubMed] [Google Scholar]
- Bind MA; Baccarelli A; Zanobetti A; Tarantini L; Suh H; Vokonas P; Schwartz J Air pollution and markers of coagulation, inflammation, and endothelial function: associations and epigene-environment interactions in an elderly cohort. Epidemiology 2012;23:332–340 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brennan SL; Pasco JA; Urquhart DM; Oldenburg B; Wang Y; Wluka AE Association between socioeconomic status and bone mineral density in adults: a systematic review. Osteoporosis Int. 2011;22:517–527 [DOI] [PubMed] [Google Scholar]
- Chan EH-W; So H-M; Tang B-S; Wong W-S Private space, shared space and private housing prices in Hong Kong: An exploratory study. Habitat Int. 2008;32:336–348 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coombes E; Jones AP; Hillsdon M The relationship of physical activity and overweight to objectively measured green space accessibility and use. Soc Sci Med. 2010;70:816–822 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Keijzer C; Tonne C; Sabia S; Basagana X; Valentin A; Singh-Manoux A; Anto JM; Alonso J; Nieuwenhuijsen MJ; Sunyer J; Dadvand P Green and blue spaces and physical functioning in older adults: Longitudinal analyses of the Whitehall II study. Environ Int. 2019;122:346–356 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Census and Statistics Department. Domestic Households by Type of Housing, 2006, 2011, and 2016 (E103). 2017. Available on: https://www.bycensus2016.gov.hk/en/bc-mt.html?search=E103 (Accessed on January 23, 2021)
- Du Y; Zhao LJ; Xu Q; Wu KH; Deng HW Socioeconomic status and bone mineral density in adults by race/ethnicity and gender: the Louisiana osteoporosis study. Osteoporosis Int. 2017;28:1699–1709 [DOI] [PubMed] [Google Scholar]
- Dzhambov AM; Browning M; Markevych I; Hartig T; Lercher P Analytical approaches to testing pathways linking greenspace to health: A scoping review of the empirical literature. Environ Res. 2020;186:109613. [DOI] [PubMed] [Google Scholar]
- Evensen KH; Hemsett G; Nordh H Developing a place-sensitive tool for park-safety management experiences from green-space managers and female park users in Oslo. Urban For Urban Gree. 2021;60:127057 [Google Scholar]
- Evenson KR; Block R; Diez Roux AV; McGinn AP; Wen F; Rodriguez DA Associations of adult physical activity with perceived safety and police-recorded crime: the Multi-ethnic Study of Atherosclerosis. Int J Behav Nutr Phys Act. 2012;9:146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fan J; Guo Y; Cao Z; Cong S; Wang N; Lin H; Wang C; Bao H; Lv X; Wang B; Gao Y; Chen Y; Yang T; Wang L; Wang C; Ruan Z; Fang L Neighborhood greenness associated with chronic obstructive pulmonary disease: A nationwide cross-sectional study in China. Environ Int. 2020;144:106042. [DOI] [PubMed] [Google Scholar]
- Feizabad E; Hossein-Nezhad A; Maghbooli Z; Ramezani M; Hashemian R; Moattari S Impact of air pollution on vitamin D deficiency and bone health in adolescents. Arch Osteoporos. 2017;12:34. [DOI] [PubMed] [Google Scholar]
- Fuertes E; Jarvis D Complex interplay between greenness and air pollution in respiratory health. Thorax. 2021; [DOI] [PubMed] [Google Scholar]
- Herzog TR; Kutzli GE Preference and Perceived Danger in Field/Forest Settings. Environ Behav. 2002;34:819–835 [Google Scholar]
- HKPD. Land Utilization in Hong Kong 2019. Hong Kong: Hong Kong Planning Department.; 2019. Available on: https://www.pland.gov.hk/pland_en/info_serv/statistic/landu.html (Accessed on January 23, 2021) [Google Scholar]
- Huang WZ; Yang BY; Yu HY; Bloom MS; Markevych I; Heinrich J; Knibbs LD; Leskinen A; Dharmage SC; Jalaludin B; Morawska L; Jalava P; Guo Y; Lin S; Zhou Y; Liu RQ; Feng D; Hu LW; Zeng XW; Hu Q; Yu Y; Dong GH Association between community greenness and obesity in urban-dwelling Chinese adults. Sci Total Environ. 2020;702:135040. [DOI] [PubMed] [Google Scholar]
- Jackson J; Stafford M Public Health and Fear of Crime: A Prospective Cohort Study. Br J Criminol. 2009;49:832–847 [Google Scholar]
- Jansson M; Fors H; Lindgren T; Wiström B Perceived personal safety in relation to urban woodland vegetation – A review. Urban For Urban Gree. 2013;12:127–133 [Google Scholar]
- Ji JS; Zhu A; Bai C; Wu CD; Yan L; Tang S; Zeng Y; James P Residential greenness and mortality in oldest-old women and men in China: a longitudinal cohort study. Lancet Planetary Health. 2019;3:e17–e25 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ji JS; Zhu A; Lv Y; Shi X Interaction between residential greenness and air pollution mortality: analysis of the Chinese Longitudinal Healthy Longevity Survey. Lancet Planetary Health. 2020;4:e107–e115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klompmaker JO; Hoek G; Bloemsma LD; Gehring U; Strak M; Wijga AH; van den Brink C; Brunekreef B; Lebret E; Janssen NAH Green space definition affects associations of green space with overweight and physical activity. Environ Res 2018;160:531–540 [DOI] [PubMed] [Google Scholar]
- Kwok T; Khoo CC; Leung J; Kwok A; Qin L; Woo J; Leung PC Predictive values of calcaneal quantitative ultrasound and dual energy X ray absorptiometry for non-vertebral fracture in older men: results from the MrOS study (Hong Kong). Osteoporosis Int. 2012;23:1001–1006 [DOI] [PubMed] [Google Scholar]
- Kwok TCY; Su Y; Khoo CC; Leung J; Kwok A; Orwoll E; Woo J; Leung PC Predictors of non-vertebral fracture in older Chinese males and females: Mr. OS and Ms. OS (Hong Kong). J Bone Miner Metab. 2017;35:330–337 [DOI] [PubMed] [Google Scholar]
- Lee AC; Maheswaran R The health benefits of urban green spaces: a review of the evidence. J Public Health. 2011;33:212–222 [DOI] [PubMed] [Google Scholar]
- Lee SB; Park Y; Kim DW; Kwon JW; Ha JW; Yang JH; Lee BH; Suk KS; Moon SH; Kim HS; Lee HM Association between mortality risk and the number, location, and sequence of subsequent fractures in the elderly. Osteoporosis Int. 2021;32:233–241 [DOI] [PubMed] [Google Scholar]
- Lin J; Leung J; Yu B; Woo J; Kwok T; Ka-Lun Lau K Socioeconomic status as an effect modifier of the association between built environment and mortality in elderly Hong Kong Chinese: A latent profile analysis. Environ Res 2021;195:110830. [DOI] [PubMed] [Google Scholar]
- Lin JS; Chan FY; Leung J; Yu B; Lu ZH; Woo J; Kwok T; Lau KK Longitudinal Association of Built Environment Pattern with Physical Activity in a Community-Based Cohort of Elderly Hong Kong Chinese: A Latent Profile Analysis. Int J Environ Res Public Health. 2020;17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu JJ; Fu SB; Jiang J; Tang XL Association between outdoor particulate air pollution and the risk of osteoporosis: a systematic review and meta-analysis. Osteoporosis Int. 2021; [DOI] [PubMed] [Google Scholar]
- Lu Z; Lam FMH; Leung JCS; Kwok TCY The U-Shaped Relationship Between Levels of Bouted Activity and Fall Incidence in Community-Dwelling Older Adults: A Prospective Cohort Study. J. Gerontol. Ser. A-Biol. Sci. Med. Sci 2020;75:e145–e151 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo YN; Huang WZ; Liu XX; Markevych I; Bloom MS; Zhao T; Heinrich J; Yang BY; Dong GH Greenspace with overweight and obesity: A systematic review and meta-analysis of epidemiological studies up to 2020. Obes Rev. 2020;21:e13078. [DOI] [PubMed] [Google Scholar]
- Maas J; Verheij RA; Spreeuwenberg P; Groenewegen PP Physical activity as a possible mechanism behind the relationship between green space and health: a multilevel analysis. BMC Public Health. 2008;8:206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Markevych I; Schoierer J; Hartig T; Chudnovsky A; Hystad P; Dzhambov AM; de Vries S; Triguero-Mas M; Brauer M; Nieuwenhuijsen MJ; Lupp G; Richardson EA; Astell-Burt T; Dimitrova D; Feng X; Sadeh M; Standl M; Heinrich J; Fuertes E Exploring pathways linking greenspace to health: Theoretical and methodological guidance. Environ Res. 2017;158:301–317 [DOI] [PubMed] [Google Scholar]
- Mazzucchelli R; Crespi Villarias N; Perez Fernandez E; Durban Reguera ML; Garcia-Vadillo A; Quiros FJ; Guzon O; Rodriguez Caravaca G; Gil de Miguel A Short-term association between outdoor air pollution and osteoporotic hip fracture. Osteoporosis Int. 2018;29:2231–2241 [DOI] [PubMed] [Google Scholar]
- Miralles-Guasch C; Dopico J; Delclos-Alio X; Knobel P; Marquet O; Maneja-Zaragoza R; Schipperijn J; Vich G Natural Landscape, Infrastructure, and Health: The Physical Activity Implications of Urban Green Space Composition among the Elderly. Int J Environ Res Public Health. 2019;16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morton B; Harper E An introduction to the Cape d'Aguilar Marine Reserve, Hong Kong. Hong Kong University Press, HKU; 1995 [Google Scholar]
- Nichol J; Wong MS; Fung C; Leung KKM Assessment of Urban Environmental Quality in a Subtropical City Using Multispectral Satellite Images. Environ Plan B Plan Des. 2006;33:39–58 [Google Scholar]
- Nilsson M; Eriksson J; Larsson B; Oden A; Johansson H; Lorentzon M Fall Risk Assessment Predicts Fall-Related Injury, Hip Fracture, and Head Injury in Older Adults. J. Am. Geriatr. Soc 2016;64:2242–2250 [DOI] [PubMed] [Google Scholar]
- Oh TK; Song IA Exposure to Air Pollution and Risk of Hip Fracture: A Population-Based Cohort Study With a 6-Year Follow-Up in South Korea. J. Occup. Environ. Med 2020;62:1034–1039 [DOI] [PubMed] [Google Scholar]
- Prada D; López G; Solleiro-Villavicencio H; Garcia-Cuellar C; Baccarelli AA Molecular and cellular mechanisms linking air pollution and bone damage. Environ Res. 2020;185:109465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prada D; Zhong J; Colicino E; Zanobetti A; Schwartz J; Dagincourt N; Fang SC; Kloog I; Zmuda JM; Holick M; Herrera LA; Hou L; Dominici F; Bartali B; Baccarelli AA Association of air particulate pollution with bone loss over time and bone fracture risk: analysis of data from two independent studies. Lancet Planetary Health. 2017;1:e337–e347 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qi J; Ruan Z; Qian ZM; Yin P; Yang Y; Acharya BK; Wang L; Lin H Potential gains in life expectancy by attaining daily ambient fine particulate matter pollution standards in mainland China: A modeling study based on nationwide data. PLoS Med. 2020;17:e1003027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qiao D; Pan J; Chen G; Xiang H; Tu R; Zhang X; Dong X; Wang Y; Luo Z; Tian H; Mao Z; Huo W; Zhang G; Li S; Guo Y; Wang C Long-term exposure to air pollution might increase prevalence of osteoporosis in Chinese rural population. Environ Res. 2020;183:109264. [DOI] [PubMed] [Google Scholar]
- Ranzani OT; Milà C; Kulkarni B; Kinra S; Tonne C Association of Ambient and Household Air Pollution With Bone Mineral Content Among Adults in Peri-urban South India. JAMA Netw. Open 2020;3:e1918504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rees-Punia E; Hathaway ED; Gay JL Crime, perceived safety, and physical activity: A meta-analysis. Prev. Med 2018;111:307–313 [DOI] [PubMed] [Google Scholar]
- Rojas-Rueda D; Nieuwenhuijsen MJ; Gascon M; Perez-Leon D; Mudu P Green spaces and mortality: a systematic review and meta-analysis of cohort studies. Lancet Planetary Health. 2019;3:e469–e477 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Su Y; Leung J; Hans D; Lamy O; Kwok T The added value of trabecular bone score to FRAX(R) to predict major osteoporotic fractures for clinical use in Chinese older people: the Mr. OS and Ms. OS cohort study in Hong Kong. Osteoporosis Int. 2017;28:111–117 [DOI] [PubMed] [Google Scholar]
- Sung JH; Kim K; Cho Y; Choi S; Chang J; Kim SM; Kim SR; Lee G; Son JS; Park SM Association of air pollution with osteoporotic fracture risk among women over 50 years of age. J. Bone Miner. Metab 2020;38:839–847 [DOI] [PubMed] [Google Scholar]
- Tang NL; Liao CD; Ching JK; Suen EW; Chan IH; Orwoll E; Ho SC; Chan FW; Kwok AW; Kwok T; Woo J; Leung PC Sex-specific effect of Pirin gene on bone mineral density in a cohort of 4000 Chinese. Bone 2010;46:543–550 [DOI] [PubMed] [Google Scholar]
- Teixeira A; Gabriel R; Quaresma L; Alencoao A; Martinho J; Moreira H Obesity and Natural Spaces in Adults and Older People: A Systematic Review. J. Phys. Act. Health 2021:1–14 [DOI] [PubMed] [Google Scholar]
- Tian F; Qi J; Wang L; Yin P; Qian ZM; Ruan Z; Liu J; Liu Y; McMillin SE; Wang C; Lin H; Zhou M Differentiating the effects of ambient fine and coarse particles on mortality from cardiopulmonary diseases: A nationwide multicity study. Environ Int. 2020;145:106096. [DOI] [PubMed] [Google Scholar]
- van Heeswijck T; Paquet C; Kestens Y; Thierry B; Morency C; Daniel M Differences in associations between active transportation and built environmental exposures when expressed using different components of individual activity spaces. Health Place 2015;33:195–202 [DOI] [PubMed] [Google Scholar]
- Vijayakumar R; Büsselberg D.J.J.o.L.; Science GH Osteoporosis: An under-recognized public health problem: Local and global risk factors and its regional and worldwide prevalence. J Local Global Health Sci. 2016;2016:2 [Google Scholar]
- Wang D; Lau KKL; Yu R; Wong SYS; Kwok TTY; Woo J Neighbouring green space and mortality in community-dwelling elderly Hong Kong Chinese: a cohort study. Bmj Open 2017;7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Washburn RA; Smith KW; Jette AM; Janney CA The Physical-Activity Scale for the Elderly (Pase) - Development and Evaluation. J Clin Epidemiol. 1993;46:153–162 [DOI] [PubMed] [Google Scholar]
- Winstead ML; Clegg DJ; Heidel RE; Ledderhof NJ; Gotcher JE Fall-Related Facial Trauma: A Retrospective Review of Fracture Patterns and Medical Comorbidity. J Oral Maxillofac Surg. 2021;79:864–870 [DOI] [PubMed] [Google Scholar]
- Yang Y; Qi J; Ruan Z; Yin P; Zhang S; Liu J; Liu Y; Li R; Wang L; Lin H Changes in Life Expectancy of Respiratory Diseases from Attaining Daily PM2.5 Standard in China: A Nationwide Observational Study. The Innovation 2020;1:100064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu R; Leung J; Woo J Incremental predictive value of sarcopenia for incident fracture in an elderly Chinese cohort: results from the Osteoporotic Fractures in Men (MrOs) Study. J Am Med Dir Assoc. 2014;15:551–558 [DOI] [PubMed] [Google Scholar]
- Yuan Y; Huang F; Lin F; Zhu P; Zhu P Green space exposure on mortality and cardiovascular outcomes in older adults: a systematic review and meta-analysis of observational studies. Aging Clin. Exp. Res 2020; [DOI] [PubMed] [Google Scholar]
- Yuen JWM; Chang KKP; Wong FKY; Wong FY; Siu JYM; Ho HC; Wong MS; Ho JYS; Chan KL; Yang L Influence of Urban Green Space and Facility Accessibility on Exercise and Healthy Diet in Hong Kong. Int J Environ Res Public Health. 2019;16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeng Q; Li N; Wang Q; Feng J; Sun D; Zhang Q; Huang J; Wen Q; Hu R; Wang L; Ma Y; Fu X; Dong S; Cheng X The Prevalence of Osteoporosis in China, a Nationwide, Multicenter DXA Survey. J Bone Miner Res. 2019;34:1789–1797 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Characteristics of participants and bone mineral density over the study period
Table S2. Baseline characteristics of participants by quartiles (Q) of green space (500-m buffer)
Table S3. Baseline characteristics for participants with and without follow-up information on bone mineral density
Table S4. Sensitivity analysis for associations of green space with annual change in bone mineral density (mg/cm3) over 14 years
Table S5. Sensitivity analysis for associations of green space with incident fracture in the Mr. OS and Ms. OS Study.
Figure S1. Geographical distribution of the participants’ baseline addresses by quartiles (Q) of green space.