
Figure 1.
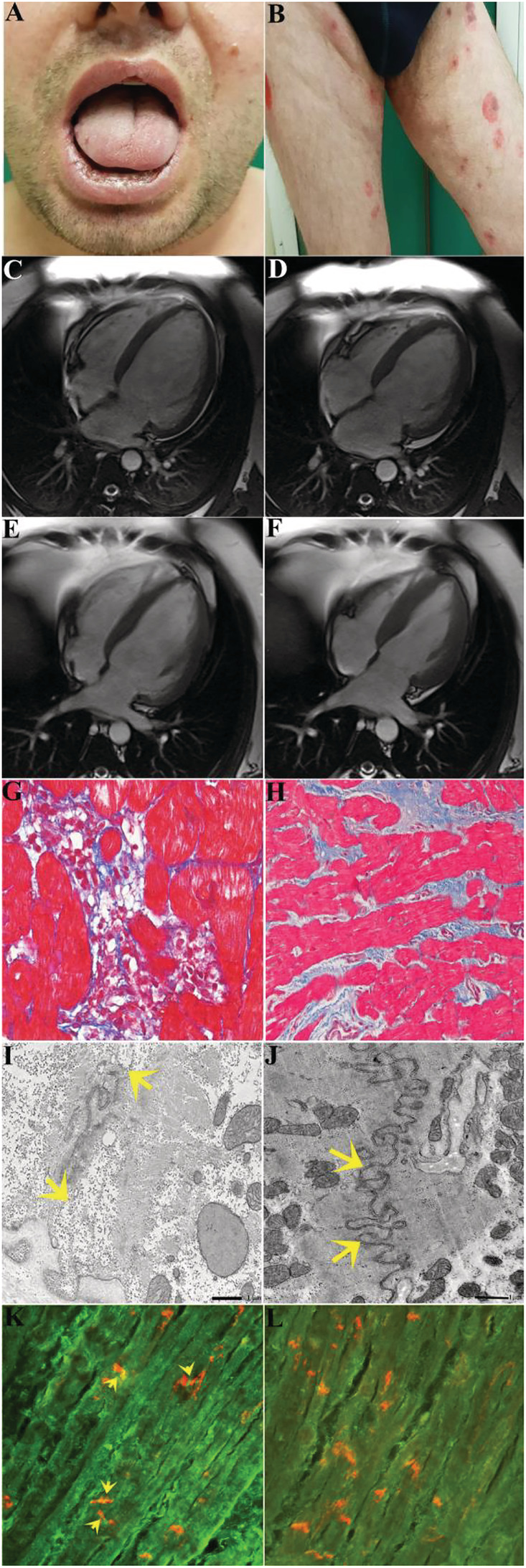
Clinical–histologic findings of pemphigus vulgaris‐associated autoimmune myocarditis before and after immunosuppression therapy. (A and B) Oral and skin lesions caused by pemphigus vulgaris. (C–F) Cardiac magnetic resonance images showing cardiac dilatation [end‐diastolic volume/body surface area (BSA) and end‐systolic volume/BSA: 154 and 119 mL/m2, respectively] and dysfunction (left ventricular ejection fraction: 22%), which recovers at 2 months of follow‐up (end‐diastolic volume/BSA and end‐systolic volume/BSA: 95.18 and 52.65 mL/m2, respectively) with left ventricular ejection fraction of 45% following immunosuppressive therapy. (G and H) Left ventricular endomyocardial biopsy before (G) and after immunosuppression (H) showing active lymphocytic myocarditis progressing to healed phase. (I) Detail of a disorganized intercalated disc. Between the arrows, residual junctional complexes are still visible. The bar represents 1 μm. (J) After therapy, the recovery of the intercalated disc is evident, with all types of junctions well recovered in all regions of the disc. The bar represents 1 μm. (K) shows positive anti‐heart autoantibodies on human heart extended to intercalated disc (in red co‐localization with antibody anti‐n‐cadherin, yellow arrow) (400×). (L) shows negative serum for anti‐heart autoantibodies on human heart and on intercalated disc (400×).