
FIGURE 4.
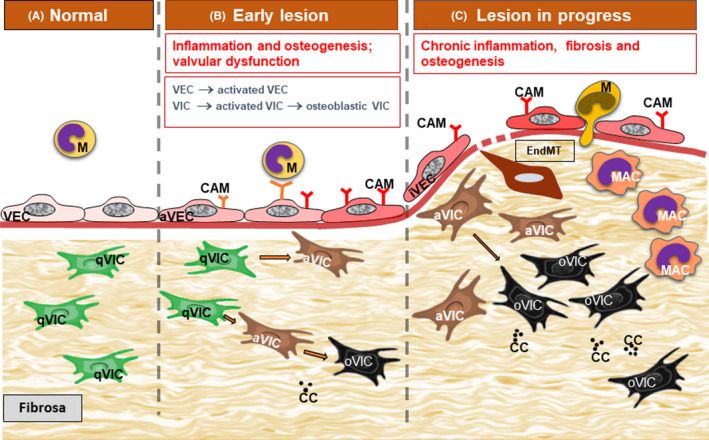
Diagram portraying diabetes‐induced accelerated progression of aortic valve atherosclerotic lesion. A. In normal conditions, valvular endothelial cells (VEC) and valvular interstitial cells (VIC) are quiescent ensuring valve homeostasis. B. The early lesion is characterized by the activation of normal VECs and the shift to a pro‐inflammatory phenotype (aVEC), the expression of new cell adhesion molecules (CAM) and subsequent monocyte (M) adhesion. VICs switch from the quiescent phenotype (qVIC) to an activated, myofibroblastic phenotype (aVIC) and an osteoblastic phenotype (oVIC). Moreover, calcification centers develop in the valvular stroma (CC). These alterations determine the onset of valvular dysfunction. C. With lesion progression, monocyte adhere and transmigrate through chronically inflamed VECs and switch to activated macrophages (MAC). Sometimes VECs undergo endothelial‐to‐mesenchymal transition (EndMT). There is an increased number of aVICs and oVICs and MAC in the valvular stroma. Chronic fibrosis develops and additional calcification centers appear, ultimately affecting valvular function